This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
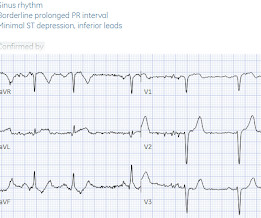
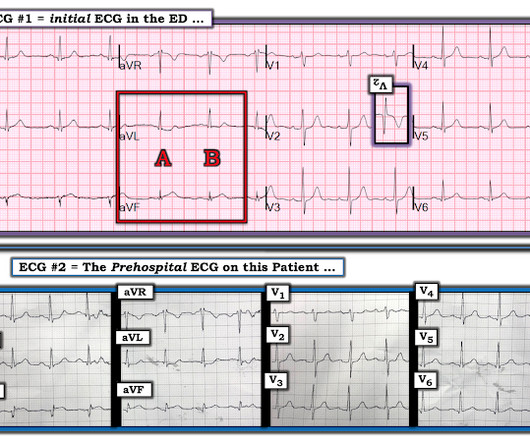
There’s sinus arrhythmia with normal conduction, normal axis and normal voltages. So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. Here’s the EMS ECG, digitized with PM cardio. What do you think?
Note the Timed Contents that I detail below facilitate finding specific material. == ECG Podcast #4 — All About Comparison ECGs for 12-Leads and Arrhythmias ( Comparing ECGs seems so "easy" to do — but so often is not done correctly! ) — published by Mayo Clinic CV Podcast Series on 5/21/2024 ( 35 minutes ). What are the problems?
And regarding arrhythmias: For more on the regular WCT — See My Comment in the May 5, 2020 post and in the April 15, 2020 post in Dr. Smith's ECG Blog. 2:25 — Dr. Grauer: The 1st Error : Too many clinicians in 2024 are still stuck in the outdated millimeter-based STEMI Paradigm”. 27:00 — SUMMARY by Dr. Anthony Kashou.
Sympathetic nerve sprouting in the infarct border zone increases transmural dispersion of repolarization, promoting arrhythmias. Overexpression of Semaphorin3A (SEMA3A), a glycoprotein regulating sympathetic nerve growth, limited ventricular arrhythmias in a rat model of MI.1
Subtle as a STEMI." (i.e., Click here to sign up for Queen of Hearts Access Here is the cardiologist's formal interpretation : "sinus rhythm with marked sinus arrhythmia, left ventricular hypertrophy with repolarization abnormality, and anteroseptal infarct, age undetermined." None of the 20 ever evolved to STEMI criteria.
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0. Large STEMI are approximately 30-80.
This includes sinus arrhythmia — in which there is often slight variation in the P-P interval. This slight variation in sinus P wave regularity tends to be greater when a 2nd- or 3rd-degree AV block is present ( called ventriculophasic sinus arrhythmia — as shown in ECG Blog #344 ). For clarity — I have done this in Figure-4.
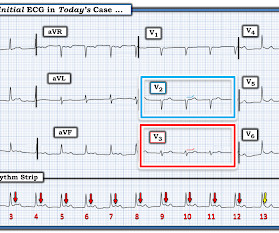
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Additionally, his cardiac telemetry monitor showed runs of accelerated idioventricular rhythm, a benign arrhythmia often associated with coronary reperfusion.
In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. In other words, the inferior "ST elevation" is due to the abnormal rhythm, and does not signify OMI or STEMI in any way. This situation has been named "Emery phenomenon." YOU TOO CAN HAVE THE PM Cardio AI BOT!!
We now have the elements needed to solve today's arrhythmia: Colored arrows in Figure-4 highlight that there is an underlying regular atrial rhythm. ECG Blog #193 — Reviews the basics for predicting the " culprit " artery ( as well as reviewing why the term "STEMI" — should be replaced by "OMI" = O cclusion-based MI ).
Whatever the specific etiology of today's arrhythmia is, the “good news” is — that this rhythm will most probably improve with reperfusion of the "culprit" artery. That said — I found today's arrhythmia fascinating, and worthy of more in-depth analysis. Using calipers facilitates the process.
Cardiac arrest #3: ST depression, Is it STEMI? Subendocardial Ischemia from some other Cause ( ie, sustained tachycardia — sinus or from some other arrhythmia; shock/profound hypotension; GI bleeding; anemia, etc. ) — or , potentially as occurred in today's case — Cardiac arrest secondary to respiratory arrest from a non-cardiac cause.
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. So there was 3-vessel disease, but with an acute posterior STEMI. There is no ST elevation. See the list below.
PEARL # 7: As is evident for many of the examples of AV block that have appeared in this ECG Blog — it is common to see a " ventriculophasic " sinus arrhythmia in association with 2nd or 3rd degree AV block. Smith’s ECG Blog. This is a free download ).
Looking at the location of ST elevation ( ie, in the inferior leads — and in V4,5,6 ) — and the location of ST depression ( ie, in leads I,aVL; V1,V2 ) — this ECG picture suggests an ongoing acute infero - postero - lateral STEMI. What is S hark F in M orphology ? Cardiopulmonary resuscitation was promptly started — but was unsuccessful.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
This was marked as "Not a STEMI" by the physicians. It is not a STEMI, but it is diagnostic of an LAD OMI (Occlusion MI). In my opinion — AI is not yet "there" with regard to interpretation of complex cardiac arrhythmias. As noted by Dr. Smith — No one could miss the acute STEMI in the repeat ECG in today's case.
Later, I found old ECGs: 5 month prior in clinic: V5 and V6 look like OMI 9 months prior in clinic with no chest symptoms: V5 and V6 look like OMI 1 year prior in the ED with chest pain: V5 and V6 sure look like a STEMI For this ECG and chest pain in the ED, the Cath lab activated. But the angiogram was clean. There was no OMI.
The computer called it a normal ECG Algorithm unknown Aside : [There is some "sinus arrhythmia", which is indeed a normal finding. Sinus arrhythmia is sinus rhythm whose rate varies with respiration. If the longest P-P interval is 120 ms greater than the shortest, it is sinus arrhythmia. Learning Points: 1.
Introduction:Atrial fibrillation (A fib) is the most common arrhythmia affecting 1-2% of the general population. Patients with documented STEMI, left ventricular thrombus, mechanical mitral or aortic valve replacement were excluded. Circulation, Volume 150, Issue Suppl_1 , Page A4140882-A4140882, November 12, 2024.
This is especially problematic in the emergency department, where computer accuracy drops as clinical significance increases—with common errors for arrhythmias and ischemia. Computer interpretation of the ECG has been called a double-edged sword: when correct, it increases physician accuracy, but when incorrect it increases errors.
Any objective, rule-based analysis of this ECG would scream "STEMI" or "OMI". And I recognized this as a STEMI mimic. Instead — my thoughts were as follows: The rhythm is sinus , with marked bradycardia and a component of sinus arrhythmia. WPW Cardiac arrhythmias ( especially AFib ). But, alas, ECGs are like faces.
Idioventricular rhythm is a common "reperfusion arrhythmia." In other words, after reperfusion therapy for STEMI, the appearance of AIVR is usually a good sign, meaning that the artery is reperfused. In fact, there may be less than 1 mm of concordant ST depression in lead V3. But it is not conclusive.
Is this inferor STEMI? Atrial Flutter with Inferior STEMI? Inferolateral ST elevation, vomiting, and elevated troponin == MY Comment , by K EN G RAUER, MD ( 5/1 /2023 ): == In my experience — Atrial Flutter ( AFlutter ) is by far, the most commonly overlooked cardiac arrhythmia. Christmas Eve Special Gift!!
There is clearly sufficient STE for STEMI criteria in leads V2 and aVL, but lead I has less than 1.0 mm of STE - thus, technically this ECG does not meet STEMI criteria, although it is a quite obvious OMI. This ECG was immediatel y discussed with the on-call cardiologist who said the ECG was "concerning but not a STEMI."
It does not meet STEMI criteria. Obvious STEMI(+) OMI of inferior, posterior, and lateral walls, now with likely 2nd degree heart block type 1 (Wenckebach). Learning Points: We can find OMI on ECG much sooner than STEMI criteria in many cases, and of course many OMIs never meet STEMI criteria at all. Easy for anyone.
Discussion See this post: STEMI with Life-Threatening Hypokalemia and Incessant Torsades de Pointes I could find very little literature on the treatment of severe life-threatening hypokalemia. IV administration of potassium is indicated when arrhythmias are present or hypokalemia is severe (potassium level of less than 2.5
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. But which myocardial walls are affected?
Although sinus arrhythmia may sometimes occur in a pattern that resembles "group beating" — I thought the difference in R-R interval duration between shorter and longer cycles in Figure-2 was much greater than would be expected with sinus arrhythmia. This left 2 additional considerations. That said — SA block is rare.
This algorithm called it a STEMI. Yet it gave a diagnosis of STEMI. This is, in effect, a transient STEMI 2. The rhythm in ECG #1 is sinus arrhythmia. It measured all the ST segments and recorded them (see bottom right) It only measure one lead (III) as greater than 1 mm, so there are not "2 leads with at least 1 mm".
Here is the repeat ECG at 52 minutes after arrival to triage: Obvious posterolateral STEMI Angiographic findings: 1. page 1932 • “The application of STEMI ECG criteria on a standard 12-lead ECG alone will miss a significant minority of patients who have acute coronary occlusion. (21) Left main: no significant stenosis.
This ECG clearly meets STEMI criteria by the way, regardless of age or gender. This is a high troponin (most STEMI are above 10 ng/mL for troponin I). MY THOUGHTS on ECG #1 ( if it was the Only Tracing I Had ): There is sinus arrhythmia ( variable R-R interval — but all p waves conducting with a constant PR interval ).
But it doesn’t meet STEMI criteria, and was not identified by the computer or the over-reading cardiologist. Still no WPW pattern, and more obvious inferoposterior OMI, but still STEMI negative. The emergency physician wasn’t sure what to make of the changes from one ECG to the next but was concerned about ACS. What do you think?
P utting I t A ll T ogether : In today's patient, who presented with chest pain ( that began the night before ) and " lightheadedness" — the ECG in Figure-3 is diagnostic of an acute STEMI ( ST E levation M yocardial I nfarction ). ECG Blog #185 — Reviews the P s, Q s, 3 R Approach to Arrhythmia Interpretation.
A "STEMI alert" was called and soon cancelled. Subendocardial Ischemia from another Cause ( ie, sustained tachycardia — sinus or from some other arrhythmia; shock/profound hypotension; GI bleeding; anemia; etc. ). There is a tiny hint of STE in aVL, but overall I do not think this looks like high lateral OMI.
Here, I do not see OMI (although the ECG is falsely STEMI positive with just over 1 mm STE in V1 and about 2.5 Never forget that sinus tachycardia is the scariest arrhythmia. What do you think? Although not necessarily intentional, the first processing that I do when I see an ECG is to categorize as OMI or not. mm STE in V2).
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. myocardial infarction), arrhythmias, valvular pathology, shunts, or outflow obstructions. What do you see?
IV administration of potassium is indicated when arrhythmias are present or hypokalemia is severe (potassium level of less than 2.5 malignant ventricular arrhythmias are present), rapid replacement of potassium is required. to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 If the patient is at 1.8,
Exclusion criteria were age less than 18, SBP less than 100 mmHg, echocardiogram with EF less than 50%, STEMI, pregnancy, and trauma. Other nonspecific findings may include P wave abnormalities, PR segment deviations, and atrial arrhythmias — though none of these findings are seen in a majority of patients.
The finding of all negative QRS complexes in leads V3-thru- V6 therefore strongly suggests that the arrhythmia-associated impulse is not traveling over an AP ( Steurer et al — Clin. This should result in at least some positivity of QRS complexes as one moves toward the lateral chest leads. Cardiol 17:306-308, 1994 ).
No arrhythmias occurred en route. Using the STEMI paradigm would have resulted in significant delays for this patient, which correspond with the doubled mortality and morbidity of NSTEMI Occlusions seen in over 50,000 subjects in NSTEMI trials. == MY Comment, by K EN G RAUER, MD ( 9/30/2019 ): == Our THANKS to Dr.
Dyspnea, Right Bundle Branch block, and ST elevation Here are two more cases where the differential diagnosis is acute OMI vs. LV aneurysm: Is this acute STEMI? Given that the patient was asymptomatic from these arrhythmias — there was time to contemplate additional measures. LV Aneurysm? Would you give Thrombolytics?
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content