This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Distribution Variance of Focal Atrial Tachycardia Foci and Long-Term Outcomes After Ablation. ABSTRACT Introduction The distribution of the origin of focal atrial tachycardia (FAT) in patients with different ages have not been clearly elucidated. After a mean follow-up of 47.2 months, FAT recurred in 57 patients.
CT of the chest showed no pulmonary embolism but bibasilar infiltrates. Even with tachycardia and a paced QRS duration of ~0.16 (And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status. She was intubated.
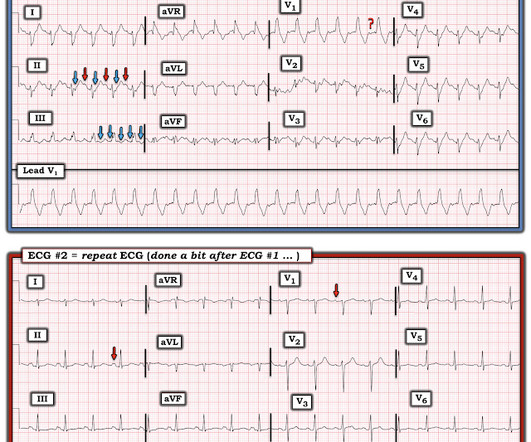
MY Initial Thoughts: In my experience — all-too-many emergency providers fail to appreciate the potential contribution that a brief ( 1-to-2 line ) history may convey when interpreting arrhythmias. when the usual negative P wave deflection of sinus tachycardia is nowhere to be found in lead V1 )? What do YOU think?
BACKGROUND:Varying rates of nonsustained ventricular tachycardia (NSVT) have been reported early after transcatheter pulmonary valve replacement (TPVR) with the Harmony valve, but data regarding rhythm outcomes beyond hospital discharge are limited.
She was awake, alert, well perfused, with normal mental status and overall unremarkable physical exam except for a regular tachycardia, possible rales at both bases, some mild RUQ abdominal tenderness. Thus, I believe it is a regular, monomorphic, wide complex tachycardia. Or it could simply still be classic VT. What is the Diagnosis?
Both atria develop from a combination of the primitive atrium, sinus venous, and pulmonary veins.It In all probability, this dilation is a form of atrial tachycardia and atrial cardiomyopathy. In contrast to other tachycardias, with atrial fibrillation (AF), the focus is often speculative, and ablation attempts are made accordingly.
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
Volta Medical has announced it has entered into a Joint Development Agreement with GE Healthcare to enhance arrhythmia procedures with artificial intelligence (AI)-driven electrophysiology technologies. 1 Approximately 33 million patients worldwide are living with AFib.
Objective We report the feasibility, safety, and clinical efficacy of focal monopolar PFA in patients with the origin of their atrial arrhythmia in the SVC. Coronary vasospasm occurred (and quickly resolved after injection of nitroglycerin) in one patient during additional ablation of a focal atrial tachycardia at the coronary sinus ostium.
Multifocal Atrial Tachycardia 2. Failure to follow this advice will undoubtedly lead to overlooking subtle acute MIs — and , it will especially lead to misdiagnosing many cardiac arrhythmias ( as was done in this case ). How can you avoid overlooking this arrhythmia? Sinus with multifocal PACs 3. Sinus with multifocal PVCs 4.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. The Initial ECG in Today's Case: As per Dr. Meyers — the initial ECG in today's case shows sinus tachycardia with bifascicular block ( = RBBB/LAHB ). Sinus Tachycardia ( common in any trauma patient. ). QTc prolongation.
Unlike paroxysmal AF, which describes symptoms that last for seven days or fewer, persistent AF is a sustained arrhythmia that lasts for more than a week 1. Early treatment of persistent AF can reduce the risk of blood clots, stroke, and heart failure, and may prevent the disease from becoming permanent.
Although the QDOT MICRO™ Catheter was mainly designed for pulmonary vein isolation (PVI) its versatility to treat atrial fibrillation (AF) and other types of arrhythmias was recently evaluated by the FAST and FURIOUS study series and other studies and will be presented in this article.
She was noted to be in heart failure, with hypotension and tachycardia. Echocardiography demonstrated severe calcific mitral stenosis with pulmonary hypertension. With decompensated heart failure and adequate prior anticoagulation, the patient underwent direct current synchronised cardioversion for her arrhythmia.
Pulsed field ablation (PFA) has become increasingly important in the treatment of cardiac arrhythmias. In addition to single-shot devices mainly used for pulmonary vein isolation, focal PFA may provide a treatment option that increases the versatility of the technique.
NOTE: For more on ECG recognition of RVH and/or pulmonary hypertension ( re the qR pattern in lead V1 ) — See ECG Blog #234 and Blog #248. Because of this, it is uncommon to see sinus tachycardia with a prolonged PR interval. Figure-3: How to assess for possible 2:1 atrial activity. = This is precisely what we see in Figure-6.
Abstract Background The newly introduced nonthermal pulsed field ablation (PFA) is a promising technology to achieve fast pulmonary vein isolation (PVI) with high acute success rates and good safety features. Compared to PFA VHPSD-PVI might ensure information on left atrial substrate allowing to target concomitant secondary tachycardias.
Extra-pulmonary vein (PV) triggers have been reported in up to 4.9-15% 15% of all atrial fibrillation (AF) patients who undergo catheter ablation and plays significant roles in arrhythmia recurrence.1,2 Extra-pulmonary vein (PV) triggers have been reported in up to 4.9-15%
The Kaplan-Meier curve of all-atrial arrhythmia-free survival for (A) all persistent patients and (B) patients who underwent PSM conducted to the higher recurrence rate in PVI + group. Conclusions PVI plus extra PV ablation using a pentaspline PFA catheter is associated with a higher incidence of atrial tachycardia recurrences.
There is a narrow complex tachycardia at a rate of 130. ECGs: there is a regular narrow complex tachycardia still at a rate of exactly 130, with no P-waves and also no change since the prehospital ECG. During tachycardia, in this case, the baseline continuously undulates especially in leads II, aVR and V1; very good for atrial flutter.
The ECG and long lead II rhythm strip in Figure-1 — was obtained from a COVID positive patient with persistent tachycardia not responding to Diltiazem. Figure-1: The initial ECG — obtained from a patient with persistent tachycardia. ( Hypoxic injury ( from pneumonia or other acute pulmonary complication ).
Backgroundwide antral pulmonary vein isolation (PVI) is effective for treating paroxysmal atrial fibrillation (PAF), although time-demanding. Procedural data and electrophysiology (EP) laboratory times were systematically collected and analyzed.
A 37-year-old woman with biventricular repair for pulmonary atresia and an intact ventricular septum was referred for an electrophysiological study in the context of recurrent atrial arrhythmias with multiple electrical cardioversions. Her clinical tachycardia was easily inducible and had a cycle length (TCL) of 340 ms.
The cyanosis in Ebstein’s anomaly, is usually not due to pulmonary hypertension, but because tricuspid regurgitation jet is directed across the atrial septal defect. This can be a source of cardiac arrhythmia as well. This is one important cause of supraventricular tachycardia in Ebstein’s anomaly.
a global leader in cardiac arrhythmia treatment and part of Johnson & Johnson MedTech , today announced European CE mark approval of the VARIPULSE Platform for the treatment of symptomatic drug refractory recurrent paroxysmal atrial fibrillation ( AF ) using pulsed field ablation (PFA). [ii] Catheter Ablation. Available at: [link].
There is sinus tachycardia. Sinus tachycardia, which exaggerates ST segments and implies that there is another pathology. I have always said that tachycardia should argue against acute MI unless there is cardiogenic shock or 2 simultaneous pathologies. Here is that ECG: What do you think? See Table for diagnostic utility.
In addition to pulmonary vein isolation (PVI), ablation of DISPERS was performed aiming at homogenizing, dissecting, isolating, or connecting DISPERS areas to nonconducting anatomical structures. ms after) and AF termination to atrial tachycardia (AT) or sinus rhythm (SR) in 12 patients (24%). to 202.2 ± 21.6 ms
Crochetage sign on ECG in ASD ECG in ASD with severe pulmonary hypertension: Tall R’ in V1, ST depression in inferior leads and V2-V5, and T inversion in inferior leads and V1-V6 are seen. Fragmented QRS is a marker of myocardial scar and consequent arrhythmias in ischemic and nonischemic cardiomyopathy.
This is the proposed mechanism of precipitation of arrhythmias in Brugada syndrome during febrile episodes. There is a potential risk for drug challenge in that life threatening ventricular arrhythmias could be precipitated. This leads to shortening of action potential duration. With proper precautions, risk can be reduced.
PEARL #2: As cited in ECG Blog #252 — my favorite truism in arrhythmia interpretation is, "The commonest cause of a pause is a blocked PAC". ECG Blog #65 — for an example of MAT in a patient with chronic pulmonary disease ( plus more on the differential diagnosis of MAT ). ECG Blog #199 and ECG Blog #366 — for Review of M AT.
Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. See here for management of Polymorphic Ventricular Tachycardia , which includes Torsades. IV administration of potassium is indicated when arrhythmias are present or hypokalemia is severe (potassium level of less than 2.5
No arrhythmias occurred en route. C linically — the rhythm we see in the long lead II of ECG #3 behaves similar to MAT, even though there is no tachycardia. A majority of patients with MAT have longstanding pulmonary disease. Rather than antiarrhythmic medication — optimizing pulmonary function is the best treatment approach.
Further ultrasound showed no B-lines (no pulmonary edema). WPW Cardiac arrhythmias ( especially AFib ). The heart rate is too fast for this poor filling. Preload must be increased and the heart rate slowed in order to allow more LV filling. These patients are often on beta blockers to prevent such a scenario.
The ECG shows sinus tachycardia, a narrow, low voltage QRS with alternating amplitudes, no peaked T waves, no QT prolongation, and some minimal ST elevation in II, III, and aVF (without significant reciprocal STD or T wave inversion in aVL). It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia.
The patient was transported to the CCU for further medical optimization where a pulmonary artery catheter was placed. myocardial infarction), arrhythmias, valvular pathology, shunts, or outflow obstructions. Furthermore, a study compared patients with AS to patients without AS in acute pulmonary edema who received nitrates.
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. The most recent and probably best study is this: Canadian Syncope Arrhythmia Risk Score. Vasovagal syncope is generally benign.
Methods Octogenarians with AF or consecutive atrial tachycardia undergoing index or re-ablation (pulmonary vein isolation [PVI] and ablation beyond PVI with different energy sources) in a single center, were analyzed. Arrhythmia-free survival at 1 year was 72.6%. Outcome data regarding CA in these patients are scarce.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. BACKGROUND:Patients undergoing first-time atrial fibrillation (AF) ablation can benefit from targeting non-pulmonary vein (PV) triggers. Preprocedural identification of high-risk individuals can guide planning of ablation strategy.
For right or wrong reasons, the world of electrophysiology has pushed us into a belief system that, if it is AF, the culprit must be pulmonary veins. In fact, non-pulmonary vein origins can be a staggering 70% in some series. If we look at the above map,RA prevails over LA convincigly in termes of focal atrial tachycardia.
ABSTRACT Introduction Freedom from recurrences of atrial tachyarrhythmia (ATA) is suboptimal after pulmonary vein isolation (PVI) in patients with persistent atrial fibrillation (PsAF). This sub-analysis from the Cryo Global Registry sought to investigate predictors of ablation success after PVI using cryoballoon ablation (CBA) for PsAF.
August 2024 Approvals Minima Stent System (P240003) (Approval Date: August 28, 2024) The Minima Stent System is an expandable cobalt-chromium metal mesh tube to reopen blood vessels in neonates, infants, and children with Coarctation of the Aorta and Pulmonary Artery Stenosis, specifically designed to expand as younger patients grow.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content