This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
New-onset arrhythmias are common in patients with chronic obstructive pulmonary disease (COPD) and obstructive sleep apnea (OSA). However, scarce data exists regarding arrhythmia risk in overlap syndrome (OS), encompassing COPD and OSA.
Specific cardiovascular diseases, such as acute myocardial infarction, arrhythmias, pulmonary hypertension and pericarditis, were also pointed. Elevated risk of arrhythmias, particularly atrial fibrillation, correlated with occupational silica exposure.
Atrial fibrillation is the most prevalent arrhythmia with a lifetime risk of nearly 30%. Pulmonary vein isolation (PVI) is the most effective treatment for rhythm control. It can be associated with reduced quality of life and complications such as heart failure and stroke.
Current guideline indications for intervention in asymptomatic patient are centred on left ventricular dimensions and ejection fraction and may include consideration in atrial fibrillation, pulmonary hypertension and those with left atrial dilatation.
Transcatheter pulmonary valve replacement (TPVR) has become a safe and effective alternative to surgical PVR in tetralogy of Fallot (TOF), isolated pulmonary stenosis (PS), and other congenital heart disease (CHD) variants.
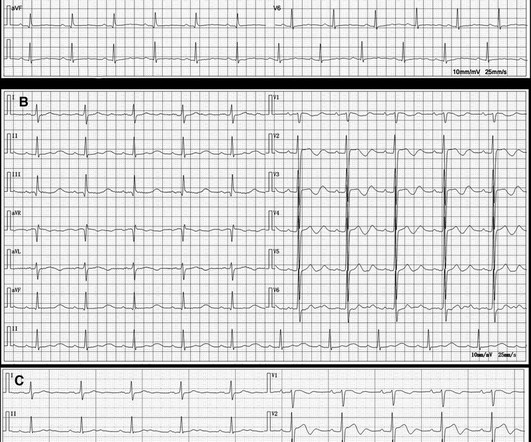
For full discussion of the case — CLICK HERE — ECG Rhythm Overview: A 12-year-old boy was admitted to our hospital with severe myocardial dysfunction and chaotic rhythm with tachy- and bradycardic arrhythmias. Perhaps the patient has pulmonary hypertension and/or tricuspid regurgitation?
At present we do not have any reliable intra-procedural electrophysiologic predictors of long-term success of AF ablation other than pulmonary vein isolation. We evaluated selected intraprocedural pulmonary vein characteristics that may be helpful in future guidance of persistent AF ablation. Results PV capture was identified in 20.3%
BackgroundAtrial dysfunction is a risk factor for atrial arrhythmia and can be detected by atrial strain imaging in patients with biventricular circulation. Newonset and recurrent atrial arrhythmias were ascertained from baseline encounter to last followup.
The results of pulmonary vein isolation are limited by arrhythmia recurrence, which is most often due to a failure to effectuate a durable contiguous circumferential transmural lesion around the pulmonary vein (PV) ostia.
Low voltage area (LVA) and low conduction velocity (CV) are promising risk factors to identify patients with abnormal atrial substrate at a high risk of atrial fibrillation (AF) recurrence following pulmonary vein isolation (PVI).
Atrial arrhythmias (AA) are common in patients with pulmonary disease and various cancers. However, the association between AA and non-small cell lung cancer (NSCLC), and the impact of AA on overall clinical outcome in patients with NSCLC are not well-known.
Figure 1 shows the chest radiograph of the first patient diagnosed with amiodarone pulmonary toxicity back in 1978.1 Amiodarone had been in use for the treatment of cardiac arrhythmias for more than a decade by the time we first identified a potential association of amiodarone therapy and pulmonary toxicity.1
Recurrent arrhythmia post PVI is most often secondary to pulmonary vein (PV) reconnections. The evidence on use of adenosine triphosphate (ATP) vs. isoproterenol (ISO) during PVI to reduce recurrence of arrhythmia is conflicting.
Patients with D-transposition of the great arteries (D-TGA) palliated with atrial switch often develop atrial arrhythmias (AA) requiring pulmonary venous atrium (PVA) access for ablation, which can be achieved via retrograde aortic approach (RAA) or trans-baffle access (TBA).13
With the advent of self-expanding transcatheter valves that can be safely deployed into the native RVOT, it is now possible to avoid repeat cardiac operations to address progressive pulmonary valve dysfunction.
Background Pulmonary vein isolation with wide antral ablation leads to better clinical outcomes for the treatment of atrial fibrillation, but the isolation lesion is invisible in conventional cryoballoon ablation. The primary outcome was a clinical recurrence of documented atrial arrhythmias for >30 s during the 1-year follow-up.
Young adults had a higher proportion of FAT originating from the superior vena cava and pulmonary veins. After a mean follow-up of 47.2 months, FAT recurred in 57 patients.
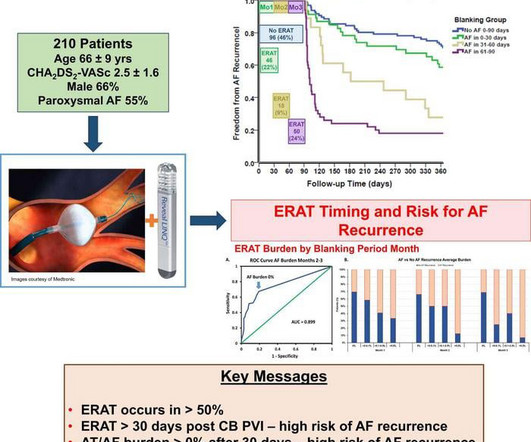
This forms the physiologic rationale for the accepted convention of a three-month blanking period, during which arrhythmia recurrences are presumed to be relatively benign and not indicative of treatment failure. However, this reasoning disregards valuable data regarding early arrhythmia recurrences and their potential significance.
Animal studies suggest that catheter ablation-associated parasympathetic and sympathetic denervation could result in increased ventricular arrhythmias (VA). The impact of catheter ablation of atrial fibrillation on VA burden in humans has not been assessed.
Objective We report the feasibility, safety, and clinical efficacy of focal monopolar PFA in patients with the origin of their atrial arrhythmia in the SVC. Conclusions In this patient cohort with SVC-triggered atrial arrhythmia, isolation using focal monopolar PFA was feasible, effective, and safe.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. BACKGROUND:High-power short-duration ablation has shown impressive efficacy and safety for pulmonary vein isolation (PVI); however, initial efficacy results with very high power short-duration ablation were discouraging. No complications occurred.
Multiple randomized controlled trials (RCTs) have compared the efficacy of pulmonary vein isolation (PVI) adjunctive techniques with PVI alone in patients with persistent atrial fibrillation (AF).
Although the QDOT MICRO™ Catheter was mainly designed for pulmonary vein isolation (PVI) its versatility to treat atrial fibrillation (AF) and other types of arrhythmias was recently evaluated by the FAST and FURIOUS study series and other studies and will be presented in this article.
Both atria develop from a combination of the primitive atrium, sinus venous, and pulmonary veins.It Spatial relationship of sites for atrial fibrillation drivers and atrial tachycardia in patients with both arrhythmias July 2017 International Journal of Cardiology 248(3) AF begets AF. Let us see few factors. References Nil ,
PVI, pulmonary vein isolation. Herein we describe the effects of catheter ablation on AF burden, arrhythmia recurrences, and ventricular function in end-stage HF. Overall, 97 patients received ablation; 66 patients (68%) underwent pulmonary vein isolation (PVI) and 31 patients (32%) were treated with PVI and additional ablation.
Unlike paroxysmal AF, which describes symptoms that last for seven days or fewer, persistent AF is a sustained arrhythmia that lasts for more than a week 1. Early treatment of persistent AF can reduce the risk of blood clots, stroke, and heart failure, and may prevent the disease from becoming permanent.
2 BB area pacing defined using P-wave criteria has been associated with decreased atrial arrhythmia burden, recurrence, and de novo incidence compared with right atrial septal pacing and right atrial appendage pacing.3
The approach for recurrent persistent AF, beyond pulmonary vein isolation, remains contentious. Despite advances, catheter ablation success rates for persistent AF remain at 50-60%. Surgical maze procedures have demonstrated superior outcomes compared to catheter ablation.
Abstract Background The newly introduced nonthermal pulsed field ablation (PFA) is a promising technology to achieve fast pulmonary vein isolation (PVI) with high acute success rates and good safety features. Two tamponades occurred in the PFA while in VHPSD two pts suffered groin bleedings.
Pulmonary vein isolation (PVI) has been established as a cornerstone therapy for atrial fibrillation (AF). 1 Several studies have highlighted the significant role of non-pulmonary premature atrial complexes (non-PV PACs) in triggering AF/AT episodes.2,3
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. The primary end point was any documented atrial arrhythmia lasting 30 seconds after a 3-month blanking period after ablation. to 3.4%]; hazard ratio, 0.66 [95% CI, 0.460.94]).
1 PFA is conventionally used for pulmonary vein isolation (PVI), but interest has arisen in delivering linear lesions to the posterior wall2 and mitral isthmus.3 Pulsed field ablation (PFA) is a novel modality shown to be safe and efficient.1 3 The durability of these lesion sets has not been well evaluated.
AF research predominantly focuses on the LA due to two key paradigms: Firstly, the well-established view that AF onset is primarly triggered by activity originating in the pulmonary veins (PVs) of the LA [1].
This novel cryoballoon with adjustable size and low compliance successfully achieves pulmonary vein isolation to treat paroxysmal atrial fibrillation (PAF), providing more options for patients with PAF. This cryoballoon system was proven to be safe and effective for treatment of patients with drug refractory or drug intolerant PAF.
BackgroundAmiodarone is a class III antiarrhythmic drug that is commonly used in the clinic to treat ventricular arrhythmias and atrial fibrillation. However, its long-term use is associated with serious adverse effects, including thyroid dysfunction, liver injury, and pulmonary toxicity, necessitating careful monitoring and management.
We present real-world 5-year follow-up data of AI-guided pulmonary vein isolation. The probability of freedom from atrial arrhythmia with repeat procedures is as follows: year 1: 0.95, year 2: 0.92, year 3: 0.85, year 4: 0.79, and year 5: 0.72. of patients remaining free from atrial arrhythmia at 1 year and 72.3%
Abstract Introduction Pulmonary vein isolations (PVI) are being performed using a high-power, short-duration (HPSD) strategy. The primary endpoint was the 1-year recurrence of any atrial arrhythmia lasting ≥30 s, detected using three 14-day ambulatory continuous ECG monitoring. Procedural and safety endpoints were also evaluated.
This middle-aged patient presented with SOB, weakness, and mild pulmonary edema. In my experience the aspect of interpretation that computer algorithms do most poorly in, is interpretation of complex arrhythmias. She previously had Atrial fibrillation with LBBB. Here is her ED ECG: Does this reveal the etiology of her symptoms?
Pulsed field ablation (PFA) has become increasingly important in the treatment of cardiac arrhythmias. In addition to single-shot devices mainly used for pulmonary vein isolation, focal PFA may provide a treatment option that increases the versatility of the technique.
Echocardiography demonstrated severe calcific mitral stenosis with pulmonary hypertension. With decompensated heart failure and adequate prior anticoagulation, the patient underwent direct current synchronised cardioversion for her arrhythmia.
CT of the chest showed no pulmonary embolism but bibasilar infiltrates. (And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status. She was intubated. Bedside cardiac ultrasound showed moderately decreased LV function.
Abstract Introduction During atrial fibrillation ablation (AFA), achievement of first pass isolation (FPI) reflects effective lesion formation and predicts long-term freedom from arrhythmia recurrence. We aim to determine the clinical and procedural predictors of pulmonary vein FPI.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content