This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
PR depression, which suggests pericarditis 4. We also showed that, of 47 cases of pericarditis with ST elevation, none had ST depression in aVL. ) Exclusion criteria were age less than 18, SBP less than 100 mmHg, echocardiogram with EF less than 50%, STEMI, pregnancy, and trauma. Absence of any ST depression in aVL. (
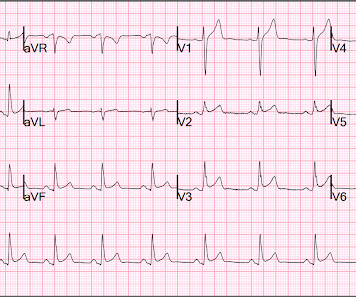
This ECG clearly meets STEMI criteria by the way, regardless of age or gender. Haven't you been taught that this favors pericarditis? Weren't you taught that concave morphology favors pericarditis? This is a high troponin (most STEMI are above 10 ng/mL for troponin I). There is no STE or STD in III an aVF.
If you were thinking that this is not anterior OMI because there is no reciprocal ST depression , it is important to remember that half of anterior STEMI do NOT have any reciprocal ST depression. Pericarditis? If you were thinking that this is pericarditis, that would be possible in the absence of any clinical information.
Note: according to the STEMI paradigm these ECGs are easy, but in reality they are difficult. Theres inferior STE which meets STEMI criteria, but this is in the context of tall R waves (18mm) and relatively small T waves, and the STD/TWI in aVL is concordant to the negative QRS. This was false positive STEMI with an ECG mimicking OMI.
ECG met STEMI criteria and was labeled STEMI by computer interpretation. While traditionally described as “benign early repolarization”, they have been associated with J wave syndromes along with Brugada syndrome, causing ventricular arrhythmias (1, 2). Take home : Not all STEs are STEMIs or OMIs. What do you think?
Smith : I recognize this as a STEMI mimic. Overnight telemetry showed no arrhythmias ( important to reduce the risk of worrisome arrhythmia given this patient's chief complaint of sudden syncope without prodrome ). Here is his ECG: There is significant ST Elevation in inferior leads, with reciprocal ST depression in aVL.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content