This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Primary endpoint was the incidence of patients with new onset supraventricular arrhythmia (AF, atrial flutter or any supraventricular tachycardia) lasting >30s, post PFO closure.ResultsA total of 59 patients met the inclusion criteria. A total of 88 supraventricular arrhythmia events (96.6% days (IQR 1321). days (IQR 1321).
Interpreting the waves and detecting abnormalities: Typically, the heart conducts electricity in a pathway starting in the sinoatrial node (SA), our heart’s “natural pacemaker”, located in the wall of the right atrium. Sinus tachycardia – sinus rhythm above 100 bpm is a sinus tachycardia.
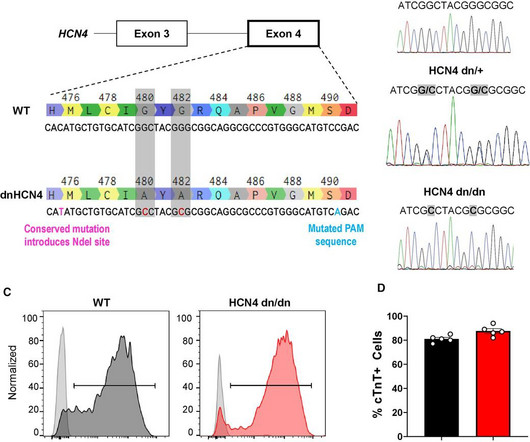
BackgroundHuman pluripotent stem cell-derived cardiomyocytes (hPSC-CMs) show tremendous promise for cardiac regeneration following myocardial infarction (MI), but their transplantation gives rise to transient ventricular tachycardia (VT) in large-animal MI models, representing a major hurdle to translation.
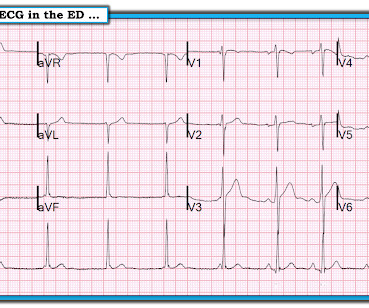
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
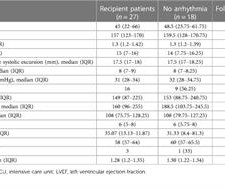
111.87), arrhythmias were detected in 9 (33%) patients. Three patients developed symptomatic sinus node dysfunction at 18, 25, and 38 days and received permanent pacemakers. One patient developed a complete AV block during acute rejection at 76 months and received a temporary pacemaker. On a median follow-up of 35.07
Place temporary pacemaker 3. Even with tachycardia and a paced QRS duration of ~0.16 Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. See this post: How a pause can cause cardiac arrest 2. Discontinue amiodarone, since it prolongs the QT 4. J Am Coll Cardiol.
Many patients with mild to moderately reduced left ventricular ejection fraction (LVEF) that require permanent pacemaker (PPM) implantation do not have a concurrent indication for implantable cardioverter-defibrillator (ICD) therapy. However, the risk of ventricular tachycardia/fibrillation (VT/VF) in this population is unknown.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. During early childhood, 50% of patients develop multifocal atrial tachycardia, a treatment-resistant tachyarrhythmia of unknown pathogenesis. HCN inhibitors targeted pacemaker-like activity in mutant ACMs. Automated patch clamping assessed funny currents.
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. It is hard to make out P waves but you can see them best in V2, and notches in the T waves in other leads - this is a sinus tachycardia with a very long PR interval indicating first degree block.
Refers to: “PVC response Atrial-Pace,” an algorithm designed for preventing pacemaker-induced tachycardia after premature ventricular contractions, triggers atrial high rate episodes.1
BackgroundScreening for atrial fibrillation (AF) may reveal incidental arrhythmias of relevance. We furthermore report treatment decisions because of incidental arrhythmias. We furthermore report treatment decisions because of incidental arrhythmias. We found incidental arrhythmias in 94 patients (11.8%).
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
This can initiate ventricular arrhythmias like polymorphic ventricular tachycardia (PMVT). Given the LV-RV offset of 40 msec, she would have received these two tightly coupled pacemaker spikes in an asynchronous mode, in this unfortunate instance during her T wave. Telemetry showed pacer spikes initiating PMVT.
It's a very "fun" ECG, with initial ectopic atrial tachycardia (negative P waves in inferior leads conducting 1:1 with the QRSs), followed by spontaneous resolution to sinus rhythm. What About the Tachycardia? Today's regular SVT rhythm could be an ectopic atrial tachycardia ( ATach ) — or an automatic junctional tachycardia.
Atrioventricular block (AVB) is a frequent initial presentation of cardiac sarcoidosis (CS), but dangerous ventricular arrhythmias (VA) can occur. Despite the scarcity of data, guidelines recommend ICD rather than a pacemaker implantation whenever a device is needed.
Multifocal Atrial Tachycardia 2. MAT has at least 3 distinct P-wave morphologies, but there is no single dominant pacemaker (i.e., Failure to follow this advice will undoubtedly lead to overlooking subtle acute MIs — and , it will especially lead to misdiagnosing many cardiac arrhythmias ( as was done in this case ).
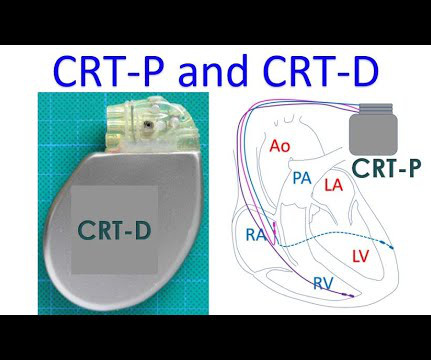
CRT is a type of pacemaker in which three chambers of the heart are paced, right atrium, right ventricle and left ventricle. The timing of the stimuli given by the pacemaker is adjusted to produce synchrony of contractions of the left ventricle. This picture illustrates what reduced ejection fraction means.
We admitted him for probable EP study and possible pacemaker. He underwent pacemaker placement and is doing fine. SSS is by far the most common reason for permanent pacemaker placement. during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. Learning Points: 1.
The ECG and long lead II rhythm strip in Figure-1 — was obtained from a COVID positive patient with persistent tachycardia not responding to Diltiazem. Figure-1: The initial ECG — obtained from a patient with persistent tachycardia. ( MAT is not a Wandering Pacemaker. How would YOU interpret this tracing?
== P EARL # 1: The easiest way to instantly enhance your arrhythmia interpretation skills is by using calipers. The cardiologist who does not regularly use calipers for interpretation of complex arrhythmias is a cardiologist who will miss the diagnosis on more than a few occasions. Using calipers will NOT slow you down.
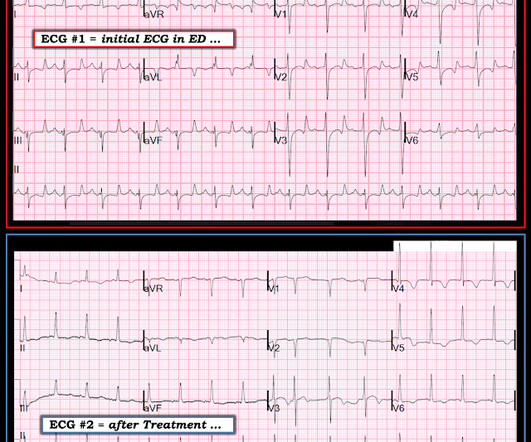
Figure-2: We have labeled ECG #2 to explain the rhythm ( See text ). == Clinically — Brief appearance of a coronary sinus rhythm until a PAC reset the sinus pacemaker did not affect outcome in this case. Failure to do so may affect clinical outcome in other cases.
Arrhythmias : A leadless pacemaker-defibrillator system provides antitachycardia pacing for ventricular tachycardia in patients with subcutaneous ICDs. Coronary Heart Disease : Initiate beta-blockers in patients with acute MI and normal LVEF unless contraindicated or if they have heart failure.
Most of the time with AV block — the atrial rhythm will be regular ( or at least almost regular — if there is an underlying sinus arrhythmia ). PEARL # 5: As noted above — today's arrhythmia appears to represent some form of 2nd-degree AV block. Figure-4: I needed to draw a laddergram.
This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute. since sleep apnea is a readily treatable cause of nighttime bradycardia, as well as of other arrhythmias ). No pause beyond 2.0
PEARL #2: As cited in ECG Blog #252 — my favorite truism in arrhythmia interpretation is, "The commonest cause of a pause is a blocked PAC". ECG Blog #200 — for an example of Wandering Atrial Pacemaker. The September 30, 2019 post in Dr. Smith’s ECG Blog — for an example of “MAT”, but without the tachycardia.
Therefore, she underwent temporary pacemaker placement and overdrive pacing at a rate of 90 bpm to keep the heart rate up in order to prevent these PVCs triggering ventricular arrhythmia. Hypokalemia was unlikely because she continued to have ventricular arrhythmia despite of correcting electrolytes.
No arrhythmias occurred en route. It is also not a wandering pacemaker — because change in atrial pacing site is gradual with that disorder. C linically — the rhythm we see in the long lead II of ECG #3 behaves similar to MAT, even though there is no tachycardia. He was loaded with aspirin, ticagrelor, and heparin.
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. Isoprenalin was discontinued, and a temporary transveous pacemaker was implanted. The patient stabilized following pacemaker placement. VT is the second most common presenting arrhythmia.
There are three mechanisms of arrhythmia: automatic, re-entry, and triggered. The most common triggered arrhythmia is Torsades de Pointes. Automatic activity refers to enhanced pacemaking function (typically from a non sinus node source), for example atrial tachycardia. What is the rhythm? References: Ferrier, G.
However, he suddenly developed a series of malignant ventricular arrhythmias. This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). Below are printouts of some of the arrhythmias recorded. What do you think?
Introduction The incidence of arrhythmia in heart failure with non-reduced ejection fraction (HFnon-rEF) in patients who have a history of hospitalisation is unclear. Methods and analysis This is a multicentre single arm study to evaluate the usefulness of ILR for detecting arrhythmia.
Methods Octogenarians with AF or consecutive atrial tachycardia undergoing index or re-ablation (pulmonary vein isolation [PVI] and ablation beyond PVI with different energy sources) in a single center, were analyzed. Arrhythmia-free survival at 1 year was 72.6%. Outcome data regarding CA in these patients are scarce.
Clinical studies have shown healthy females have faster baseline and intrinsic sinoatrial node (SAN) rhythm than males, potentially leading to SAN tachycardia, suggesting sex-specific expression of pacemaker ion channels including L- and T-type Ca2+ channels.
Among 299 patients with CRT-pacemakers (BVP-111, LBBAP-188), VT/VF occurred in 8 patients in the BVP group vs. none in the LBBAP group (7.2% Physiologic resynchronization by LBBAP may be associated with lower risk of arrhythmias compared with BVP. The occurrence of VT/VF was significantly lower with LBBAP compared with BVP (4.2%
Arrhythmia In simple words, arrhythmia refers to an irregular heartbeat. A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. ECG testing is also carried out to see how medicines work during treatment and the pacemaker's functioning.
How does a pacemaker accomplish RBBB morphology? Quick aside on device terminology (feel free to skip): A "single chamber" pacemaker is a device with only one lead. A "dual chamber" pacemaker is a device with an atrial lead and a ventricular lead. So the most likely rhythm in ECG 1 is ectopic atrial tachycardia.
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. The most recent and probably best study is this: Canadian Syncope Arrhythmia Risk Score. Syncope with Exertion (EGSYS) 7. Baumann, B.
The CASE Continues: The patient had many episodes of NSVT ( Non-Sustained Ventricular Tachycardia ) — like th e one shown below in Figure-6. So, we are looking for signs of an underlying regular atrial rhythm ( with perhaps slight sinus arrhythmia ) — and it is much easier to find this when you know what you are looking for! (
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content