This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
UC San Diego Health is the first in San Diego to successfully implant the world’s first dual chamber and leadless pacemaker system to help treat people with abnormal heart rhythms. Holding the device and pictured above is Ulrika Birgersdotter-Green, MD, cardiologist and director of pacemaker and ICD services at UC San Diego Health.
Fadi Mansour performed the first Canadian implant of BIOTRONIK ’s newest pacemaker and CRT-P generation earlier this year at the Centre Hospitalier de l'Université de Montréal. The patient received an Amvia Sky HF-T QP triple chamber pacemaker device. Atrial arrhythmia management tools, including atrial antitachycardia pacing (ATP).
Primary endpoint was the incidence of patients with new onset supraventricular arrhythmia (AF, atrial flutter or any supraventricular tachycardia) lasting >30s, post PFO closure.ResultsA total of 59 patients met the inclusion criteria. A total of 88 supraventricular arrhythmia events (96.6% days (IQR 1321). days (IQR 1321).
BackgroundThere have been few instances of symptomatic bradycardia-arrhythmia in the context of area postrema syndrome (APS), and some of them have been implanted permanent pacemakers. Brady-arrhythmia was presented in all patients, and 9 patients were implanted temporary or permanent pacemakers.
A pacemaker modified for newborns' tiny bodies safely and effectively stabilized their heart rhythms for up to two years, according to new research published in Circulation: Arrhythmia and Electrophysiology.
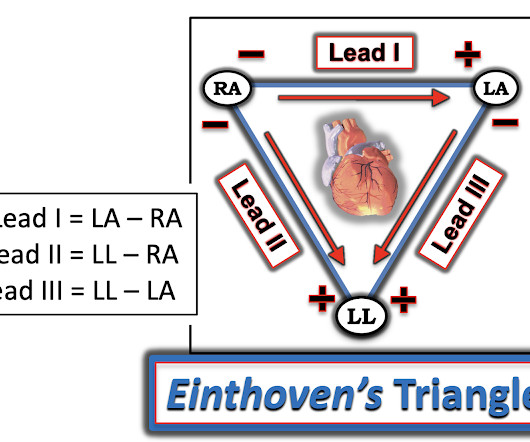
Interpreting the waves and detecting abnormalities: Typically, the heart conducts electricity in a pathway starting in the sinoatrial node (SA), our heart’s “natural pacemaker”, located in the wall of the right atrium. 1] Arrhythmia Recognition: The Art of Interpretation, T.Garcia, D.Garcia. Usually does not exceed 160 bpm.
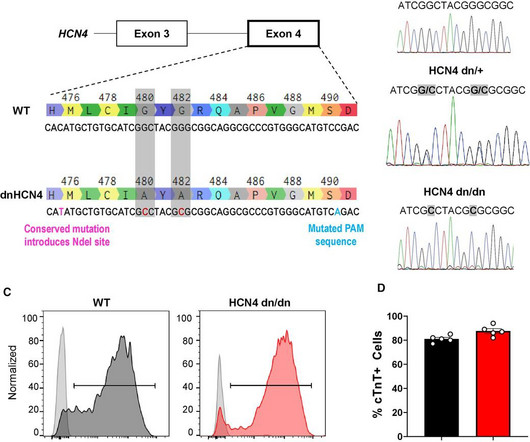
ConclusionsWhile genetic silencing of the pacemaker ion channel HCN4 suppresses the automaticity of hPSC-CMs in vitro, this intervention is insufficient to reduce VT risk post-transplantation in the pig MI model, implying more complex mechanism(s) are operational in vivo.
A heart attack is a life-threatening condition, with patients remaining at risk of premature death long after the actual attack—50% to 60% of patients die subsequently as a result of sudden cardiac death, triggered by cardiac arrhythmia.
For full discussion of the case — CLICK HERE — ECG Rhythm Overview: A 12-year-old boy was admitted to our hospital with severe myocardial dysfunction and chaotic rhythm with tachy- and bradycardic arrhythmias. In the meantime, a pacemaker may be needed. = Hope this helps — :) ECG-3 — I see sinus bradycardia and arrhythmia.
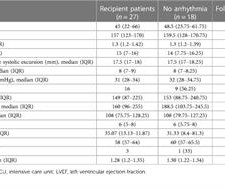
111.87), arrhythmias were detected in 9 (33%) patients. Three patients developed symptomatic sinus node dysfunction at 18, 25, and 38 days and received permanent pacemakers. One patient developed a complete AV block during acute rejection at 76 months and received a temporary pacemaker. On a median follow-up of 35.07
Pacemaker malfunction maybe life threatening by inducing malignant arrhythmia or failure to pace in dependent patients. We report a case of syncope and injury related to device malfunction, where the only solution was exchanging the pacemaker generator.
Background Cardiac arrhythmias have markedly increased in recent decades, highlighting the urgent need for appropriate test systems to evaluate the efficacy and safety of new pharmaceuticals and the potential side effects of established drugs.
External electric cardioversion (ECV) effectively converts atrial and ventricular arrhythmias and is also recommended for patients with cardiovascular implantable electronic devices (CIED) (1, 2).
Cardiac accumulation triggers local tissue injury, electrical instability and arrhythmia. Objective We conducted a systematic review evaluating AF burden and bradycardia requiring permanent pacemaker (PPM) implantation and report any predictive risk factors identified. Age was associated with AF (OR 1.05–1.20
Written by Willy Frick A man in his 70s with a history of HFrEF and sick sinus syndrome s/p dual chamber pacemaker placement was admitted for overnight observation following outpatient placement of a mitral valve clip. This is unambiguous evidence of pacemaker malfunction. Imagine the pacemaker is set at a minimum rate of 60.
Cardiac arrhythmias are often encountered in orthotopic heart transplantation (OHT) recipients due to multiple risk factors and may lead to the necessity of permanent pacemaker implantation(PPI). Ischemic time > 4 hours has been associated with graft dysfunction.
Is a pacemaker needed? With P waves labeled — Isn't it now much easier to appreciate that the atrial rhythm is quite regular ( with no more than a slight sinus arrhythmia )? P utting I t A ll T ogether : The precise mechanism of today's arrhythmia is complex and difficult to determine. Is this " high -grade" AV block?
Many patients with mild to moderately reduced left ventricular ejection fraction (LVEF) that require permanent pacemaker (PPM) implantation do not have a concurrent indication for implantable cardioverter-defibrillator (ICD) therapy. However, the risk of ventricular tachycardia/fibrillation (VT/VF) in this population is unknown.
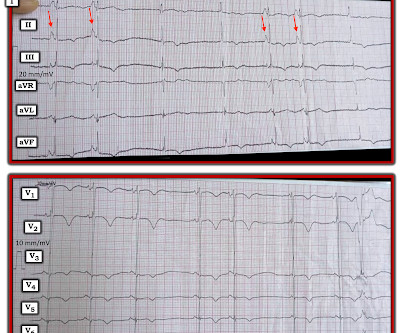
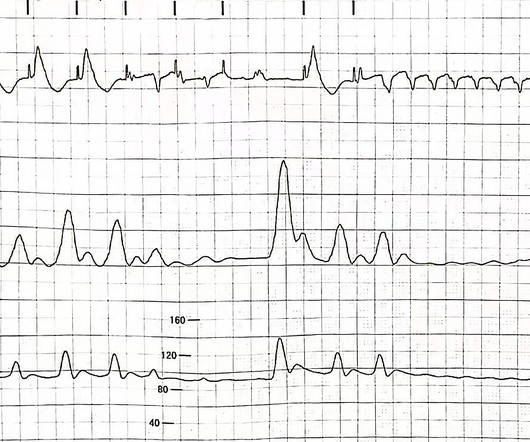
However, he suddenly developed a series of malignant ventricular arrhythmias. Below are printouts of some of the arrhythmias recorded. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. The arrhythmia starts with a PVC having a short coupling interval.
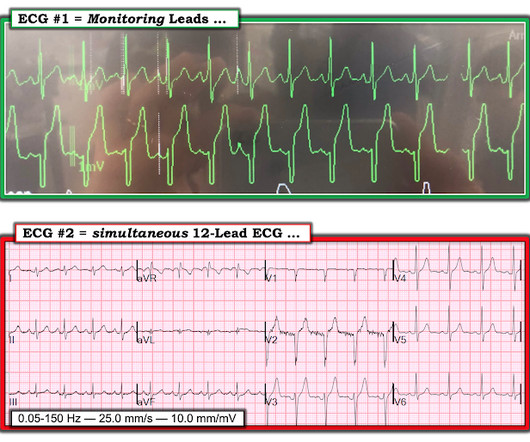
Written by Willy Frick A woman in her 90s with a history of end stage renal disease and complete heart block status post dual chamber pacemaker presented from home with acute onset dyspnea. As per Dr. Frick — pacemaker spikes are best seen in lead aVL of ECG #1. ECG is shown below. What do you think?
A cardiac arrhythmia is an abnormal heartbeat caused by a problem in the "wiring" of your heart muscle. You may or may not feel it but it should not be ignored.
BackgroundScreening for atrial fibrillation (AF) may reveal incidental arrhythmias of relevance. We furthermore report treatment decisions because of incidental arrhythmias. We found incidental arrhythmias in 94 patients (11.8%). Journal of the American Heart Association, Ahead of Print. of our cohort patients.
Refers to: “PVC response Atrial-Pace,” an algorithm designed for preventing pacemaker-induced tachycardia after premature ventricular contractions, triggers atrial high rate episodes.1
They knew she would need a pacemaker unless some transient and reversible cause was discovered. Once this happens, of course, the patient will require temporary or permanent pacemaker as soon as possible. She required intermittent pacing from the temp wire numerous times overnight so a permanent pacemaker was placed the next day.
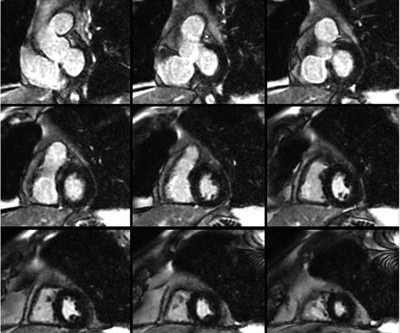
Workup including echocardiography, cardiac magnetic resonance imaging, and Holter monitor did not show evidence of ACM or significant arrhythmias. He underwent urgent dual chamber pacemaker implantation, during which a ventricular programmed stimulation study was performed and was negative for sustained ventricular arrhythmias.
There are three mechanisms of arrhythmia: automatic, re-entry, and triggered. The most common triggered arrhythmia is Torsades de Pointes. Automatic activity refers to enhanced pacemaking function (typically from a non sinus node source), for example atrial tachycardia. This has been discussed many times before on this blog.
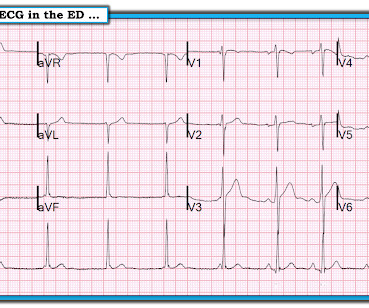
Here is the first ED ECG: COMPUTER INTERPRETATION: Electronic Atrial Pacemaker. He has a h/o 3rd degree heart block and has a pacemaker. His pacemaker was interrogated and it was found that the pacemaker was not adquately capturing. Lethal arrhythmias may be a terminal event ( VT/VFib; Asystole ). The K was 5.8
At CTVS, our team of board-certified thoracic surgeons routinely perform a procedure known as a thoracic sympathectomy to treat hyperhidrosis, or excessive sweating. During this surgery, part of the sympathetic chain of nerves that runs along the spine is carefully severed to halt signals that trigger the sweat glands.
Electrical storm (ES) is a clinical emergency characterized by multiple malignant ventricular arrhythmias or ICD discharges within 24 h, requiring early rational management.
This patient does not have a pacemaker, so this must be a ventricular escape rhythm. Redundant and diverse intranodal pacemakers and conduction pathways protect the human sinoatrial node from failure. The KEY to interpreting many complex arrhythmias lies with determination of what is and what is not a P wave. & Fedorov, V.
LBBAP significantly improved LVEF without causing fatal ventricular arrhythmias. All patients had a reduced LVEF of 36%–50% and underwent pacemaker implantation. No fatal ventricular arrhythmias occurred. Conclusion LBBAP significantly improved cardiac systolic dysfunction without causing fatal ventricular arrhythmias.
Introduction The incidence of arrhythmia in heart failure with non-reduced ejection fraction (HFnon-rEF) in patients who have a history of hospitalisation is unclear. Methods and analysis This is a multicentre single arm study to evaluate the usefulness of ILR for detecting arrhythmia.
Massie Block -Ref 1) But, if there is something unusual in the clinical history, be ready to investigate until the arrhythmia, or at least the anxiety disappears. Final message AV blocks, even Mobitz type 2, can occur at normal times of heightened vagal tone.( Reference 1.
The rapid technological advancements in cardiac implantable electronic devices such as pacemakers, implantable cardioverter defibrillators, and loop recorders, coupled with a rise in the number of patients with these devices, necessitate an updated clinical framework for periprocedural management.
Atrioventricular block (AVB) is a frequent initial presentation of cardiac sarcoidosis (CS), but dangerous ventricular arrhythmias (VA) can occur. Despite the scarcity of data, guidelines recommend ICD rather than a pacemaker implantation whenever a device is needed.
Pacemaker implantation combined with atrioventricular node ablation (AVNA) is a well-established strategy for non-controlled atrial arrhythmias. Limited amount of data is available regarding His Bundle Pacing (HBP), or Left Bundle Branch Area Pacing (LBBAP) in this setting.
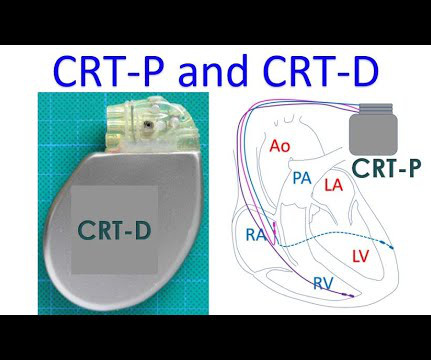
CRT is a type of pacemaker in which three chambers of the heart are paced, right atrium, right ventricle and left ventricle. The timing of the stimuli given by the pacemaker is adjusted to produce synchrony of contractions of the left ventricle. This picture illustrates what reduced ejection fraction means.
Place temporary pacemaker 3. Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. See this post: How a pause can cause cardiac arrest 2. Discontinue amiodarone, since it prolongs the QT 4. Discontinue all QT proloning medications, including azithromycin 6.
Sick sinus syndrome (SSS) is a common condition resulting in reduced quality of life, syncope, and pacemaker (PPM) implantation, but predictors have not been elucidated.
Sick sinus syndrome (SSS) is a common condition resulting in reduced quality of life, syncope, and pacemaker (PPM) implantation, but predictors have not been elucidated.
Pathogenic genetic variants in the HCN4 (hyperpolarisation-activated and cyclic nucleotide-gated channel) gene can cause sinus node dysfunction, disrupting the function of the pacemaker region of the heart. Patients with such variants can present with a wide spectrum of arrhythmias but sudden death is generally considered rare.
== P EARL # 1: The easiest way to instantly enhance your arrhythmia interpretation skills is by using calipers. The cardiologist who does not regularly use calipers for interpretation of complex arrhythmias is a cardiologist who will miss the diagnosis on more than a few occasions. Using calipers will NOT slow you down.
We admitted him for probable EP study and possible pacemaker. He underwent pacemaker placement and is doing fine. SSS is by far the most common reason for permanent pacemaker placement. during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. Learning Points: 1.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content