This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
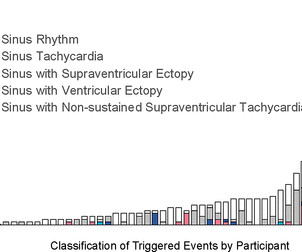
Background Cardiac arrhythmias have been observed among patients hospitalised with acute COVID-19 infection, and palpitations remain a common symptom among the much larger outpatient population of COVID-19 survivors in the convalescent stage of the disease. Participants were instructed to trigger the monitor for palpitations.
Even with tachycardia and a paced QRS duration of ~0.16 In this specific case, Left Bundle Branch (LBB) area pacing was pursued to achieve cardiac resynchronization. (J J Am Coll Cardiol. second I immediately knew there is no way this relative increase in QT duration ( compared to the R-R interval ) is going to be "normal".
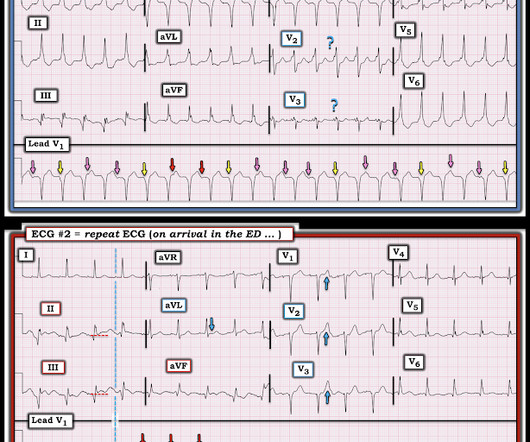
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Hopefully a repeat echocardiogram will be performed outpatient. The Initial ECG in Today's Case: As per Dr. Meyers — the initial ECG in today's case shows sinus tachycardia with bifascicular block ( = RBBB/LAHB ).
It's a very "fun" ECG, with initial ectopic atrial tachycardia (negative P waves in inferior leads conducting 1:1 with the QRSs), followed by spontaneous resolution to sinus rhythm. Hopefully his outpatient EP appointment will understand and correct that. What About the Tachycardia? Triage ECG: What do you think? was discovered.
There is a regular wide complex tachycardia. Remember : Adenosine is safe in Regular Wide Complex Tachycardia. Rather, from this one: Very Fast Very Wide Complex Tachycardia Ideally, one would cardiovert. PEARL #1: The most commonly overlooked arrhythmia is AFlutter ( A trial F lutter ).
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. It is hard to make out P waves but you can see them best in V2, and notches in the T waves in other leads - this is a sinus tachycardia with a very long PR interval indicating first degree block.
Cardioversion is used to correct abnormal heart rhythms, also known as arrhythmias. Electrical cardioversion may be recommended for you if you have certain types of arrhythmias, such as: Atrial fibrillation (AFib): This is the most common type of arrhythmia, and it can cause symptoms like dizziness, fatigue, and difficulty breathing.
Follow-up contained regular visits at our outpatient clinic at 1, 3, 6, and 12 months including 7-day Holter electrocardiograms. ms after) and AF termination to atrial tachycardia (AT) or sinus rhythm (SR) in 12 patients (24%). After a blanking period of 6 weeks, recurrence of any atrial arrhythmia was documented in 26 patients (52%).
Laurent Fiorina, Cardiovascular Institute Paris-Sud (ICPS) and medical advisor for Philips, said: “Our main focus is developing new AI models to detect cardiovascular conditions or predict future cardiac events like atrial fibrillation, ventricular tachycardia, and now, severe bradyarrhythmia.”
Case sent by Magnus Nossen MD, edits by Meyers A previously healthy woman in her 60s presented to an outpatient clinic for palpitations. The ECG there reportedly showed an irregular tachycardia, and the patient was immediately referred to the emergency room. Vitals were within normal limits other than heart rate.
This is an arrhythmia until proven otherwise. This proves AV dissociation, and by extension ventricular tachycardia. The note lists a diagnosis of "tachycardia," which is described as "narrow complex." (The Repeat ECG obtained in ER: Fortunately for the patient, his ventricular tachycardia spontaneously resolved.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content