This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
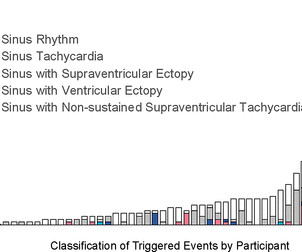
Background Cardiac arrhythmias have been observed among patients hospitalised with acute COVID-19 infection, and palpitations remain a common symptom among the much larger outpatient population of COVID-19 survivors in the convalescent stage of the disease. Participants were instructed to trigger the monitor for palpitations.
Ambulatory cardiac monitors are utilized to diagnose arrhythmias and to establish symptom-arrhythmia correlation. However, the impact of monitoring on acute clinical management decisions utilizing mobile cardiac outpatient telemetry (Philips MCOT) is not known.
Neuromodulation of the autonomic nerve system may be an effective therapeutic option for suppressing refractory ventricular arrhythmias (VAs). Given the transient effect of SGP, it is difficult to perform SGP in an outpatient setting.
Hopefully a repeat echocardiogram will be performed outpatient. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). NOTE: Prediction of cardiac contusion "severity" on the basis of cardiac arrhythmias and ECG findings — is an imperfect science. No cardiac MRI was done.
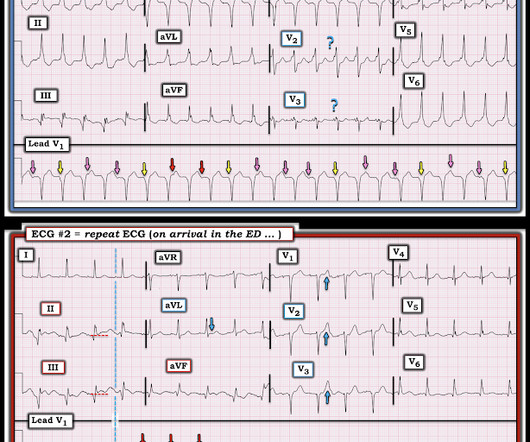
She was discharged with plan for outpatient cardiac MRI for further evalution. The "good news" ( from an arrhythmia interpretation perspective ) — is that we now see P waves much better than we did in the initial ECG. That said, for readers with an interest in complex arrhythmias — Isn't this series of serial tracings fascinating! =
Cardioversion is used to correct abnormal heart rhythms, also known as arrhythmias. Electrical cardioversion may be recommended for you if you have certain types of arrhythmias, such as: Atrial fibrillation (AFib): This is the most common type of arrhythmia, and it can cause symptoms like dizziness, fatigue, and difficulty breathing.
At this point, there was no improvement in LV function and he was out of the convalescent phase of his MI, so the decision was made to install an ICD for arrhythmia prophylaxis. An echocardiogram showed an EF of 20-25%. One month after ICD implantation, an EKG was taken: Notably, the T wave inversions are now resolved.
The EP-COT Trial: Impact of Emergent Physician Notifications from MCOT on Patient Outcomes While ambulatory cardiac monitors are frequently used to diagnose arrhythmias, their impact on clinical decision-making has not been extensively studied.
Follow-up contained regular visits at our outpatient clinic at 1, 3, 6, and 12 months including 7-day Holter electrocardiograms. After a blanking period of 6 weeks, recurrence of any atrial arrhythmia was documented in 26 patients (52%). Most arrhythmia recurrences were reentrant AT. After a total of 1.46 ± 0.68
PEARL #1: The most commonly overlooked arrhythmia is AFlutter ( A trial F lutter ). That said — the lack of a terminal S wave in lateral limb leads I and aVL is atypical for true RBBB conduction. As a result — We can not rule out VT on the basis of this single ECG.
If the patient does not present with syncope, then outpatient management is probably OK, with referral to cardiology. Taking a Closer LOOK : There is a fairly marked sinus arrhythmia ( RED arrows in Figure-2 ). PEARL # 1: It is common with 2nd- and 3rd-degree AV block to see a "ventriculophasic" sinus arrhythmia.
Hopefully his outpatient EP appointment will understand and correct that. MY point that is relevant to optimal arrhythmia interpretation — is to always look to see if there is a "break" in the rhythm at the onset or offset of the tachycardia — since if present, this will often tell you the specific diagnosis! was discovered.
Written by Willy Frick A man in his 70s with a history of HFrEF and sick sinus syndrome s/p dual chamber pacemaker placement was admitted for overnight observation following outpatient placement of a mitral valve clip. Cardiology was consulted, and the note said "no arrhythmias on telemetry or pacer interrogation." What do you think?
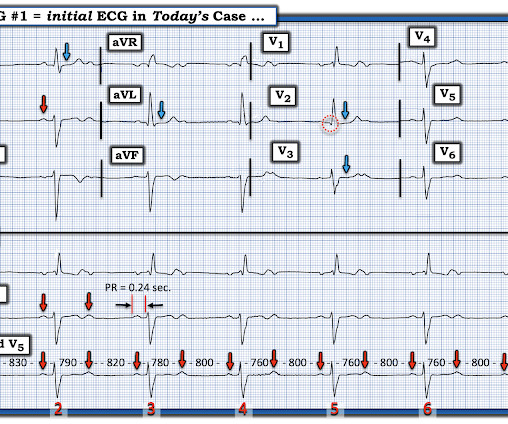
Case sent by Magnus Nossen MD, edits by Meyers A previously healthy woman in her 60s presented to an outpatient clinic for palpitations. Today's CASE: To Review — The patient in today’s case is a previously healthy woman in her 60s who was seen in an outpatient clinic for “palpitations”.
The issue is relevant since some arrhythmias are associated to sudden cardiac death occurring in young patients, and the overall risk does not cease during the early postpartum period. Both inpatients and outpatients were identified retrospectively. PVC were the most common recorder arrhythmias, followed by VF, NSVT, AF, CSD.
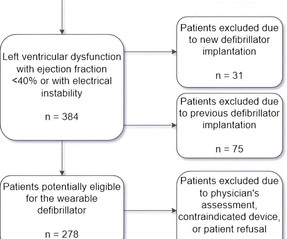
Introduction Wearable cardioverter-defibrillators (WCD) have emerged as a valuable tool in the management of patients at risk for life-threatening arrhythmias. Methods From November 2022 to May 2024, we conducted an outpatient follow-up of 41 patients receiving WCD. Among these, 12 patients (29%) underwent ICD implantation.
Arrange follow up for chest pain patients who are “STEMI negative” with “normal troponin”: the patient was referred to outpatient cardiology But 6 hours later the patient returned with recurrent chest pain: Again diagnostic of infero-posterior OMI, though this time it does STEMI criteria, albeit barely. See analysis below.
It is relevant to note here that as a physician active clinically in both the inpatient and outpatient arenas, I am an eyewitness to the severe toll COVID19 took on my patients in the Spring or 2020.
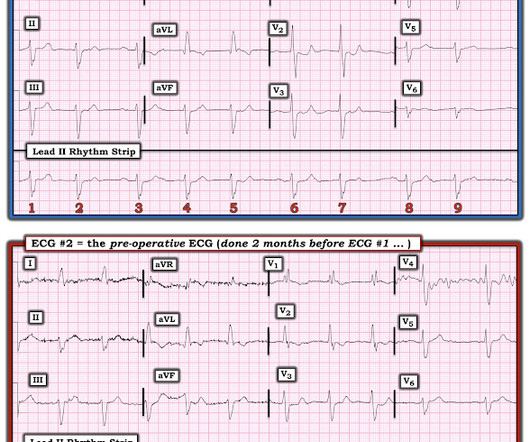
Written by Willy Frick A middle aged man presented for elective outpatient surgery. To Emphasize: For those in search of "the quick answer" — today's middle-aged man should not be approved for an outpatient elective surgical procedure without further evaluation. The following ECG was obtained in the preoperative area.
But vasovagal syncope typically has a prodrome such that further evaluation of today's patient may be needed as an outpatient to better assess for the cause of his sudden syncope. The most common cause of syncope in a previously healthy young adult like today's patient is vasovagal syncope. Troponins were negative.
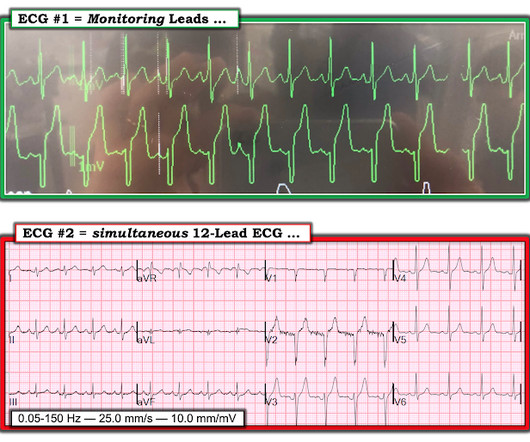
This is an arrhythmia until proven otherwise. He was discharged with a plan for outpatient PCI to his chronically occluded RCA. He complained of days to weeks of palpitations and dyspnea. His clinic ECG is shown. What do you think? In an elderly patient complaining of palpitations, we have an ECG with heart rate 140 bpm.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content