This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A prehospital 12-lead was recorded: There is a regular wide complex tachycardia. The computer diagnosed this as Ventricular Tachycardia. There is a wide complex regular tachycardia at a rate of 226. Toothache, incidental Wide Complex Tachycardia Could it be fascicular VT or Bundle Branch VT ( i.e., idiopathic VT )?
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Are you confident there is no ischemia? Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Is this: 1.
The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. The patient was brought to the ED and had this ECG recorded: What do you think? And what do you want to do?
Heart rate/rhythm: consider antidotes for brady/tachy-arrhythmias, and for sinus tachycardia consider fluids for vasodilation and benzodiazepines for agitation. Electrical conduction and axis: consider sodium bicarb for QRS > 100 especially if RBBB or terminal rightward shift, and magnesium for QTc> 500.
Ventricular tachycardia is a potentially life threatening cardiac arrhythmia. On the ECG, ventricular tachycardia can be defined as three or more ventricular ectopic beats occurring in a sequence at a rate more than 100 per minute. Another rare form of ventricular tachycardia is bidirectional ventricular tachycardia.
It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome. Even with tachycardia and a paced QRS duration of ~0.16 J Am Coll Cardiol.
A series of cardiac arrhythmias were seen during the course of her resuscitation — including the interesting arrhythmia shown in the long lead II of Figure-1. At about this point in the process — I like to take a closer LOOK at the 12-lead tracing, to ensure there is no acute ischemia or infarction that might need immediate attention.
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. The Initial ECG in Today's Case: As per Dr. Meyers — the initial ECG in today's case shows sinus tachycardia with bifascicular block ( = RBBB/LAHB ). Sinus Tachycardia ( common in any trauma patient. ).
Pediatric exercise testing may be used for evaluation of various disorders of cardiac rhythm rather than for inducible ischemia as in adults. QT prolongation and the occurrence of ventricular arrhythmias with exercise are another important aspect of exercise testing in children. Discussion on pediatric exercise testing.
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. Analysis: there is a wide complex tachycardia. This was the interpretation I put into the system: WIDE COMPLEX TACHYCARDIA. It is regular.
DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology.
There is a narrow complex tachycardia at a rate of 130. ECGs: there is a regular narrow complex tachycardia still at a rate of exactly 130, with no P-waves and also no change since the prehospital ECG. During tachycardia, in this case, the baseline continuously undulates especially in leads II, aVR and V1; very good for atrial flutter.
During active chest pain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF. Learning Points: You must learn and recognize the ECG patterns of OMI and subendocardial ischemia to best understand the ECG in acute care medicine.
Arrhythmia? Today’s case recalled that scenario for me, in that it features recognition of an arrhythmia that fooled ED staff into thinking the ECG was showing an acute infarction. The ED staff failed to do this — and as a result, they completely overlooked the arrhythmia. Would you give lytics? Yes, but not because of the ECG!
Instead, antiarrhythmic drugs such as amiodarone or ß-blockers may be needed — and/or treatment targeted to correcting ischemia. This may explain the poorer response of pleomorphic VT to antiarrhythmic therapy — and the higher morbidity and mortality that seems to be associated with this arrhythmia.
Is there ischemia? Idioventricular rhythm is a common "reperfusion arrhythmia." ECG Diagnosis is either : 1) junctional rhythm with new LBBB, and possibly ischemia 2) accelerated idoventricular rhythm with possible ischemia, and possibly related to restoration of normal perfusion. But it is not conclusive.
Precordial ST depression may be subendocardial ischemia or posterior STEMI. Notice there is tachycardia. I have warned in the past that one must think of other etiologies of ischemia when there is tachycardia. V4-V6, is much more likely to be posterior than subendocardial ischemia. There is no ST elevation.
Mechanism is thought to be due to sustained sympathetic stimulation, probably caused by dysfunction of insular cortex resulting in reversible neurogenic damage to the myocardium which could include contraction bands and subendocardial ischemia [2]. But the number of persons with lobar hemorrhage in that study was only 17%.
First, we have a narrow-complex, regular tachycardia, with a rate of about 135-140. This narrows our differential for the rhythm down to sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT, or SVT), and atrial flutter. Tachycardia and ST Elevation. She was discharged home. Christmas Eve Special Gift!!
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) This is sinus tachycardia (rhythm) with complete heart block (AV node function) with ventricular escape rate just below 30. Never forget that sinus tachycardia is the scariest arrhythmia.
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrial flutter with regular conduction. Now the patient is in sinus tachycardia. Her initial EKG is below. Adenosine worked.
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below. Arch Intern Med.
The ECG there reportedly showed an irregular tachycardia, and the patient was immediately referred to the emergency room. Here is her ECG on arrival: There is a wide complex tachycardia that is irregularly irregular (this is difficult to determine at these very high rates). Vitals were within normal limits other than heart rate.
during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. The easy way to remember the arrhythmias most commonly associated with SSS is to think of what one might expect if the SA node became sick. AFib ( Atrial Fibrillation ) is the most common sustained cardiac arrhythmia.
This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute. since sleep apnea is a readily treatable cause of nighttime bradycardia, as well as of other arrhythmias ). No pause beyond 2.0
The finding of all negative QRS complexes in leads V3-thru- V6 therefore strongly suggests that the arrhythmia-associated impulse is not traveling over an AP ( Steurer et al — Clin. Given the rapid rate of the tachycardia and the amorphous shape of the QRS — the decision was made to sedate the patient and cardiovert.
NOTE: As discussed in detail in ECG Blog #108 — " A IVR" is an "enhanced" ventricular ectopic rhythm that occurs faster than the intrinsic ventricular escape rate ( which is typically between 20-40/minute ) — but slower than hemodynamically significant Ventricular Tachycardia ( ie, VT at rates >130-140/minute ).
He has a family history concerning for arrhythmia. Given the circumstances of his car crash, we presume it was due to an underlying arrhythmia. He has a family history concerning for arrhythmia with his father requiring some sort of device (PPM, ICD, unclear) at a young age.
The finding of a fairly regular, wide tachycardia without clear sign of atrial activity ( especially when seen in an acutely symptomatic patient ) — should immediately prompt a diagnosis of VT until proven otherwise. Shark Fin" ST segment elevation is most often a sign of severe transmural ischemia that results from acute coronary occlusion.
Additionally, his cardiac telemetry monitor showed runs of accelerated idioventricular rhythm, a benign arrhythmia often associated with coronary reperfusion. Whether these EKGs show myocarditis, a normal variant, or something else, they are overall not typical of transmural ischemia of the anterior or high lateral walls.
Therefore, she underwent temporary pacemaker placement and overdrive pacing at a rate of 90 bpm to keep the heart rate up in order to prevent these PVCs triggering ventricular arrhythmia. Hypokalemia was unlikely because she continued to have ventricular arrhythmia despite of correcting electrolytes. Acute ischemia?
The ECG shows sinus tachycardia, a narrow, low voltage QRS with alternating amplitudes, no peaked T waves, no QT prolongation, and some minimal ST elevation in II, III, and aVF (without significant reciprocal STD or T wave inversion in aVL). It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia.
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. No arrhythmias occurred en route. C linically — the rhythm we see in the long lead II of ECG #3 behaves similar to MAT, even though there is no tachycardia. Repeat ECG minutes later (one shown below) showed no significant change.
In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished. 2) Tachycardia to this degree can cause ST segment changes in several ways. Again, not an expected outcome with diltiazem).
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). VT is the second most common presenting arrhythmia. She was started on isoprenalin (isoproterenol).
What is the most likely cause of this arrhythmia? IMPRESSION: Given the presence of a wide tachycardia — with 2 distinct QRS morphologies, and no sign of P waves — a presumed diagnosis of B i D irectional Ventricular Tachycardia has to be made. Acute myocardial ischemia. Figure-1: The initial ECG in today's case. (
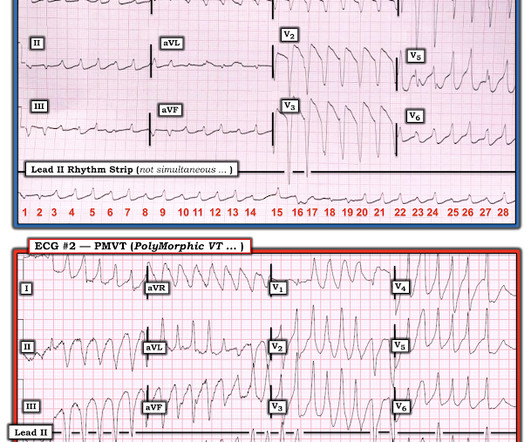
However, he suddenly developed a series of malignant ventricular arrhythmias. This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). Below are printouts of some of the arrhythmias recorded. What do you think?
There are three mechanisms of arrhythmia: automatic, re-entry, and triggered. The most common triggered arrhythmia is Torsades de Pointes. Automatic activity refers to enhanced pacemaking function (typically from a non sinus node source), for example atrial tachycardia. This has been discussed many times before on this blog.
ECG is consistent with severe hypokalemia and/or hypomagnesemia causing prolonged QT (QU) at high risk of Torsades (which is polymorphic ventricular tachycardia in the setting of a long QT interval). Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management Cardiac Arrest.
There are a number of things to look for in an ECG that can hint at arrhythmia as the cause of an apparent seizure. There is a run of polymorphic ventricular tachycardia — which given the QT prolongation, qualifies as Torsades de Points ( TdP ). Below are some of the conditions to be aware of: Preexcitation Brugada syndrome.
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
Remember, in diffuse subendocardial ischemia with widespread ST-depression there may b e ST-E in lead s aVR and V1. There are well formed R-waves with good voltage/amplitude which is uncommon for ischemia. The ECG does not show any signs of ischemia. True Positive ECG#2 : Also sinus rhythm. There is ST depression in V1.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content