This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. Cardiac arrest #3: ST depression, Is it STEMI? And what do you want to do?
The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible. Back to the assessment of ischemia: Returning to the ECG, the leads that catch my eye first are -- I, II, V4, V5, V6. For national registry purposes, this will be incorrectly classified as a STEMI.) < 0.049).
The STD maximal in V1-V4 is diagnostic of acute transmural posterior wall ischemia, most likely due to posterior OMI. Subendocardial ischemia does not localize, and subendocardial ischemia presents with STD maximal in V5-6, II, and STE in aVR. It does not meet STEMI criteria. Subendocardial ischemia does not localize.
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. I have warned in the past that one must think of other etiologies of ischemia when there is tachycardia.
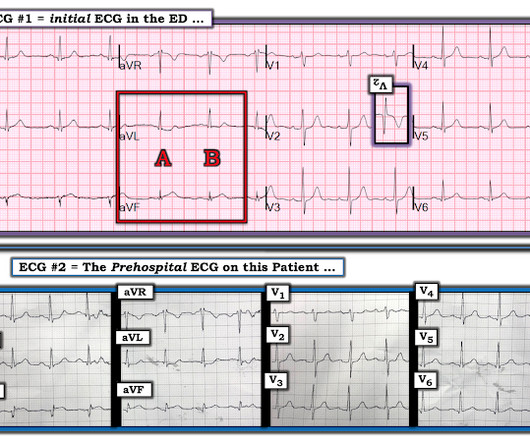
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR.
This includes sinus arrhythmia — in which there is often slight variation in the P-P interval. This slight variation in sinus P wave regularity tends to be greater when a 2nd- or 3rd-degree AV block is present ( called ventriculophasic sinus arrhythmia — as shown in ECG Blog #344 ). For clarity — I have done this in Figure-4.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.”
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Additionally, his cardiac telemetry monitor showed runs of accelerated idioventricular rhythm, a benign arrhythmia often associated with coronary reperfusion.
Is there ischemia? Idioventricular rhythm is a common "reperfusion arrhythmia." In other words, after reperfusion therapy for STEMI, the appearance of AIVR is usually a good sign, meaning that the artery is reperfused. Exactly how they relate to ischemia, chest pain, and reperfusion can only be speculated about.
This is especially problematic in the emergency department, where computer accuracy drops as clinical significance increases—with common errors for arrhythmias and ischemia. Computer interpretation of the ECG has been called a double-edged sword: when correct, it increases physician accuracy, but when incorrect it increases errors.
The precordial STD persists in severity from V4-V6, rather than being maximal in V1-V4 (as in posterior OMI), and so the ECG overall best fits the subendocardial ischemia pattern (diffuse supply/demand mismatch). A "STEMI alert" was called and soon cancelled.
The computer called it a normal ECG Algorithm unknown Aside : [There is some "sinus arrhythmia", which is indeed a normal finding. Sinus arrhythmia is sinus rhythm whose rate varies with respiration. If the longest P-P interval is 120 ms greater than the shortest, it is sinus arrhythmia.
Looking at the location of ST elevation ( ie, in the inferior leads — and in V4,5,6 ) — and the location of ST depression ( ie, in leads I,aVL; V1,V2 ) — this ECG picture suggests an ongoing acute infero - postero - lateral STEMI. What is S hark F in M orphology ? Cardiopulmonary resuscitation was promptly started — but was unsuccessful.
Learning Points: Atrial flutter can be very tricky to identify, and can cause all kinds of problems such as mimicking or concealing ischemia and OMI. Is this inferor STEMI? Atrial Flutter with Inferior STEMI? The reason for this is easy to understand — atrial activity is often not well seen in many instances of this arrhythmia.
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. But which myocardial walls are affected?
Here, I do not see OMI (although the ECG is falsely STEMI positive with just over 1 mm STE in V1 and about 2.5 In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) Never forget that sinus tachycardia is the scariest arrhythmia. What do you think?
Here was my answer: "Not ischemia. Any objective, rule-based analysis of this ECG would scream "STEMI" or "OMI". And I recognized this as a STEMI mimic. Instead — my thoughts were as follows: The rhythm is sinus , with marked bradycardia and a component of sinus arrhythmia. WPW Cardiac arrhythmias ( especially AFib ).
But it doesn’t meet STEMI criteria, and was not identified by the computer or the over-reading cardiologist. Still no WPW pattern, and more obvious inferoposterior OMI, but still STEMI negative. 2] Conduction through the accessory pathway can be intermittent (with different degrees of pre-excitation), and affected by ischemia.
The finding of all negative QRS complexes in leads V3-thru- V6 therefore strongly suggests that the arrhythmia-associated impulse is not traveling over an AP ( Steurer et al — Clin. ie, Severe subendocardial ischemia from sustained VT in a patient severe apical cardiomyopathy resulted in a peak troponin >31,000 ng/L in today's case ).
[link] Case continued: In this case, the diagnosis was much easier because there was a prehospital ECG: less than 1 mm ST Elevation in II, III, aVF, with minimal ST depression in aVL This is diagnostic of inferior OMI No clear evidence of ischemia Computer interpretation Impressive! This algorithm called it a STEMI. Learning points 1.
This ECG clearly meets STEMI criteria by the way, regardless of age or gender. Weren't you taught that "new tall T wave in V1" is concerning for ischemia, and so this is the opposite? This is a high troponin (most STEMI are above 10 ng/mL for troponin I). There is no STE or STD in III an aVF. Leads V4-V6 show new loss of S-wave.
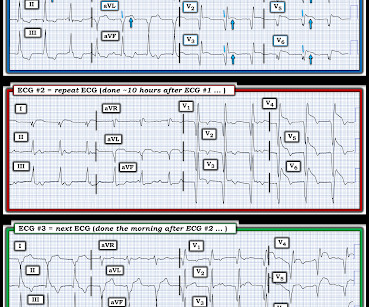
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. No arrhythmias occurred en route. The morphology in V2 is also concerning and it appears that the ST segment is being pushed down, as in ST depression. Repeat ECG minutes later (one shown below) showed no significant change.
This is ischemia until proven otherwise. This can only be due to STEMI. A fixed stenosis in that other artery, especially in the context of hypotension from the occlusion of the first coronary artery, can lead to ischemia and very poor LV function and worsening shock. By the ECG, it is not necessarily subacute, but could be.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
There are three mechanisms of arrhythmia: automatic, re-entry, and triggered. The most common triggered arrhythmia is Torsades de Pointes. It is a benign arrhythmia which requires no specific treatment. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Moffat, M.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. However, he suddenly developed a series of malignant ventricular arrhythmias. Below are printouts of some of the arrhythmias recorded. There is no definite evidence of acute ischemia. (ie, The below ECG was recorded. What do you think?
A prior ECG was available for comparison: Normal One might be tempted to interpret the ST depression as ischemia, but as Smith says, "when the QT is impossibly long, think of hypokalemia and a U-wave rather than T-wave." Is it STEMI? Instead — it commonly reflects ischemia from severe underlying coronary disease.
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct. Here is his triage ECG: There is massive STE in V3-V6, and also STE in II, III, aVF.
There’s minimal concave ST elevation in III which does not meet STEMI criteria, so this ECG is "STEMI negative". Use STEMI criteria to identify acute coronary occlusion: the ECG was STEMI negative 2. A repeat ECG was done on way to cath lab: "STEMI negative" again. The cath lab was activated. Take home 1.
V1 sits over both the RV and the septum, so transmural ischemia of either one with give OMI pattern in V1 and reciprocal STD in V5 and V6. See this post: Septal STEMI with ST elevation in V1 and V4R, and reciprocal ST depression in V5, V6. However, the pattern is also seen in inferior OMI with right ventricular OMI. (V1
If it is STEMI, it would have to be RBBB with STEMI. Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chest pain for the ischemia and potential syncope for brugada.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7]. So maybe she is better than I am. There was a 0.9%
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias. Bicarb 20, Lactate 4.2,
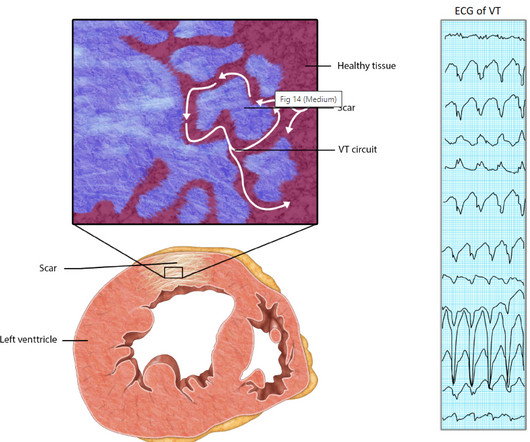
Relationship between Ischemia and arrhythmia While the relationship between Ischemia and VT is really complex, the term “Ischemic VT” itself adds more twists. Even here, it is the associated factors, like hypoxia or acidosis are the triggers which of course are resultant of Ischemia.
But it does not meet the ridiculous "STEMI criteria" since there is not 1 mm of STE in any lead. The fact that there is variation in the R-R interval for the first 4 sinus-conducted beats suggests the possibility of a marked sinus arrhythmia — but I would not expect this degree of variable P wave morphology and such group beating.
PEARL # 2: Despite the challenge of assessing a ventricular rhythm for underlying ischemia and/or infarction there are primary ST-T wave changes that are seen in Figure-3 that suggest an ongoing acute event. I represent this in the laddergam shown in Figure-6.
The rhythm is sinus ( small, but upright P wave in lead II ) with some R-R interval variability ( probable sinus arrhythmia ). When interpreting ECGs such as the initial tracing in today's case We need to remember that we are not trying to "rule in" an acute STEMI. And the initial ECG in Figure-1 is not normal.
Smith : I recognize this as a STEMI mimic. Doesn't this necessarily mean that he was having ischemia? Overnight telemetry showed no arrhythmias ( important to reduce the risk of worrisome arrhythmia given this patient's chief complaint of sudden syncope without prodrome ). I was not alarmed. Troponins were negative.
PEARL # 3: Knowing there is an acute inferior STEMI I looked next to see if there is also acute posterior involvement ( which so often accompanies inferior MI ). But larger-than-expected Q waves in each of the inferior leads ( especially in lead III ) are probably the result of this patients ongoing acute inferior STEMI.
The ECG shows sinus rhythm with normal QRS complex morphology and significant subendocardial ischemia (SEI) pattern (ST depression in many leads, worst in lateral areas including leads II, V5-6, with reciprocal STE in aVR). Here is her ECG within 30 minutes of PCI: Improved, but still with ischemia.
ECG met STEMI criteria and was labeled STEMI by computer interpretation. While traditionally described as “benign early repolarization”, they have been associated with J wave syndromes along with Brugada syndrome, causing ventricular arrhythmias (1, 2). Take home : Not all STEs are STEMIs or OMIs. What do you think?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content