This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
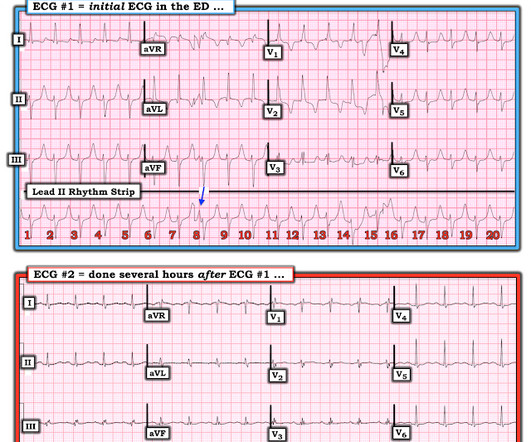
In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished. In this case, there is diffuse ischemic ST depression of subendocardial ischemia, of course with accompanying reciprocal STE in aVR.
DISCUSSION: The 12-lead EKG EMS initially obtained for this patient showed severe ischemia, with profound "infero-lateral" ST depression and reciprocal ST elevation in lead aVR. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology.
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy? How can you better assess the ST segments?
Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). VT is the second most common presenting arrhythmia. Vaso or inotropic medications are not harmless, and can precipitate life threatening arrhythmias. Usually the medical history will provide clues to the cause.
In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) The atrial rate is around 120 beats per minute, which indicates high adrenergic state and physiologic distress! Never forget that sinus tachycardia is the scariest arrhythmia. The rate is near 80, normal.
A series of cardiac arrhythmias were seen during the course of her resuscitation — including the interesting arrhythmia shown in the long lead II of Figure-1. At about this point in the process — I like to take a closer LOOK at the 12-lead tracing, to ensure there is no acute ischemia or infarction that might need immediate attention.
And superimposed subendocardial ischemia pattern, of course. While these do not alter emergency management of this patient's arrhythmia — They should be noted. It simply does not make physiologic sense to suddenly see an all-negative QRS complex in this most lateral chest lead. She was otherwise very stable during this rhythm.
2] Conduction through the accessory pathway can be intermittent (with different degrees of pre-excitation), and affected by ischemia. 3] So a patient with WPW can have the pattern induced by ischemia, and there is also a report of a patient with pre-existing WPW which was “ablated” by myocardial infarction after an LAD occlusion.[4]
We wish, our understanding about cardiac contractile physiology is deep and nearly complete. In myocardial pathology, the genesis and sustainability of ventricular arrhythmia are intricately related to the degree of LV dysfunction of any cause. (An The second reason is, NDCM is a progressive primary muscle disease.
Either could be a result of myocardial contusion There is some minimal ST depression -- this could represent ischemia What else is there that could use therapy immediately? Or, much less likely, it could be a very accelerated escape rhythm from the posterior fascicle. There is a very long ST segment resulting in a very long QT.
Evidence of acute ischemia (may be subtle) vii. Finally, much of this correlates well with The new Canadian Syncope Arrhythmia Risk Score , just published in 2016, results of which are given below in the Annotated Bibliography. The most recent and probably best study is this: Canadian Syncope Arrhythmia Risk Score. Left BBB vi.
The rhythm is sinus ( small, but upright P wave in lead II ) with some R-R interval variability ( probable sinus arrhythmia ). But the definite ST segment flattening and depression in leads V4 , V5 , V6 is real and given the history of new severe CP this has to be assumed as acute ischemia until proven otherwise.
Focus-less Atrial fibrillation Right from the days of James Mckenzie , when AF was refered to as delirium cordis or ataxia of pulse, AF was always considered as a chaotic, focus-less arrhythmia. It is still true in many cases. There are innumerable patients who develop de-novo AF without any focus. Reference 1. Francis Marchlinski Cory M.
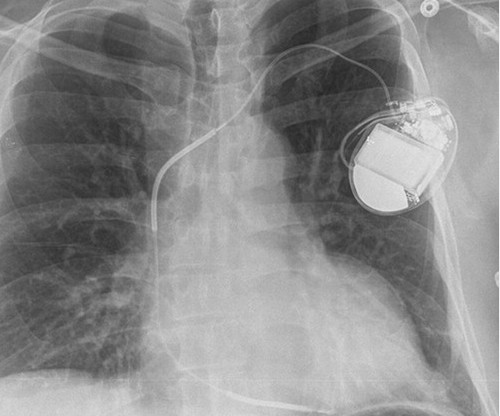
No evidence for ischemia jumps out. Conduction system pacing" is a newer technique that is being studied as a way of delivering more physiologic pacing, typically by inserting a lead into the area of the left bundle branch, or the bundle of His. But ectopic atrial tachycardia is most commonly an automatic arrhythmia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content