This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Is a pacemaker needed? With P waves labeled — Isn't it now much easier to appreciate that the atrial rhythm is quite regular ( with no more than a slight sinus arrhythmia )? P utting I t A ll T ogether : The precise mechanism of today's arrhythmia is complex and difficult to determine. Is this " high -grade" AV block?
Place temporary pacemaker 3. It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome. See this post: How a pause can cause cardiac arrest 2.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? The last echocardiography 12 months ago showed HFmrEF.
T wave alternans is characterized by variation in T-wave morphology in the setting of consistent pacemaker and QRS morphology. (1) T-wave alternans and the susceptibility to ventricular arrhythmias. Chronic amiodarone evokes no torsade de pointes arrhythmias despite QT lengthening in an animal model of acquired long-QT syndrome.
The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible. Back to the assessment of ischemia: Returning to the ECG, the leads that catch my eye first are -- I, II, V4, V5, V6. Ischemia can be disguised by a wide escape rhythm, which decreases the sensitivity of ECG.
We admitted him for probable EP study and possible pacemaker. He underwent pacemaker placement and is doing fine. SSS is by far the most common reason for permanent pacemaker placement. during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. Learning Points: 1.
My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. This suggests ischemia of uncertain duration. PEARL # 2: Interpretation of the 12-lead ECG in Figure-1 is no easy task! To EMPHASIZE: Today's laddergram was challenging.
There was no evidence of ischemia. She had a permanent pacemaker implanted. After pacer AND conversion to sinus rhythm: Computer diagnosis: IMPRESSION ELECTRONIC VENTRICULAR PACEMAKER ABNORMAL RHYTHM ECG What is missing from this interpretation? We are not told how ischemia has been ruled out in this case. Hyperkalemia.
These include: i ) Use of rate-slowing medication ( ie, ß-blockers, digoxin, verapamil/diltiazem, etc. ) ; ii ) Acute or recent infarction or ischemia; iii ) Hypothyroidism; iv ) Neurologic injury; v ) Electrolyte disturbance; and , vi ) Sleep apnea. I therefore thought the significance of this finding in today’s case was uncertain.
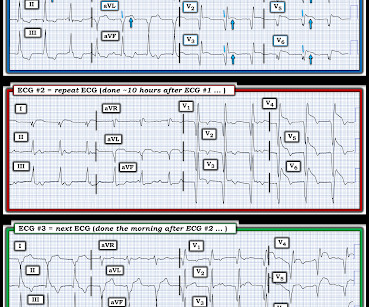
My thoughts were the following: ECGs #1 and #2 showed a completely unreliable sinus pacemaker, with presumed high-grade 2nd-degree AV block — and frequent resultant pauses of over 2 seconds ( that would have been even longer had it not been for intermittent relief from the atrial escape focus ). What Does this All Mean?
This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute. since sleep apnea is a readily treatable cause of nighttime bradycardia, as well as of other arrhythmias ).
Therefore, she underwent temporary pacemaker placement and overdrive pacing at a rate of 90 bpm to keep the heart rate up in order to prevent these PVCs triggering ventricular arrhythmia. Hypokalemia was unlikely because she continued to have ventricular arrhythmia despite of correcting electrolytes. Acute ischemia?
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. No arrhythmias occurred en route. It is also not a wandering pacemaker — because change in atrial pacing site is gradual with that disorder. Repeat ECG minutes later (one shown below) showed no significant change.
There are three mechanisms of arrhythmia: automatic, re-entry, and triggered. The most common triggered arrhythmia is Torsades de Pointes. Automatic activity refers to enhanced pacemaking function (typically from a non sinus node source), for example atrial tachycardia. This has been discussed many times before on this blog.
However, he suddenly developed a series of malignant ventricular arrhythmias. Below are printouts of some of the arrhythmias recorded. There is no definite evidence of acute ischemia. (ie, This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation.
Isoprenalin was discontinued, and a temporary transveous pacemaker was implanted. The patient stabilized following pacemaker placement. Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). VT is the second most common presenting arrhythmia.
Arrhythmia In simple words, arrhythmia refers to an irregular heartbeat. Poor blood supply Ischemia, or inadequate blood supply to the heart, is an abnormality that can be detected in an ECG test. ECG testing is also carried out to see how medicines work during treatment and the pacemaker's functioning.
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. He received a permanent pacemaker during the subsequent inpatient stay. Chapter 17: Ventricular Arrhythmias. References [1] Surawicz, B.
IMPRESSION: Today’s initial ECG is a complex tracing that manifests marked sinus bradycardia and arrhythmia — underlying RBBB — and both junctional and ventricular escape beats when the heart rate drops below 50/minute. CAVEAT: Although many of these rhythms are seen in seemingly healthy individuals — these are not always benign arrhythmias.
Evidence of acute ischemia (may be subtle) vii. Negative predictors of adverse outcome: Pacemaker Pre-syncope or "near-syncope," but there is still some small risk (5, 18) These last two are identified in studies, but I consider them dangerous signs and symptoms in their own right, as above: 10. Left BBB vi. Pathologic Q-waves viii.
No evidence for ischemia jumps out. How does a pacemaker accomplish RBBB morphology? Quick aside on device terminology (feel free to skip): A "single chamber" pacemaker is a device with only one lead. A "dual chamber" pacemaker is a device with an atrial lead and a ventricular lead. ECG 1 What do you think?
PEARL # 2: Despite the challenge of assessing a ventricular rhythm for underlying ischemia and/or infarction there are primary ST-T wave changes that are seen in Figure-3 that suggest an ongoing acute event. I represent this in the laddergam shown in Figure-6. The above said Today's patient had other ideas.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content