This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
There is limited data regarding safety, electrophysiologic characteristics and arrhythmia substrate during ventricular tachycardia (VT) ablation in patients with prior aortic valve replacement (AVR).
Ventricular tachycardia is a potentially life threatening cardiac arrhythmia. On the ECG, ventricular tachycardia can be defined as three or more ventricular ectopic beats occurring in a sequence at a rate more than 100 per minute. Another rare form of ventricular tachycardia is bidirectional ventricular tachycardia.
Establishing the precise mechanism of cardiac arrhythmias in the electrophysiology laboratory is one of the main requisites for a successful and safe ablation.
Notwithstanding many insightful observations, the electrocardiogram (ECG) arguably ignited the big bang in our understanding of cardiac arrhythmias. Using ECG recording and deductive reasoning, our teachers and predecessors classified the bradycardias and tachycardias and proposed many mechanisms, subsequently proven to be correct.
The primary end point was syncope recurrence, and the secondary end point was the reduction of the ventricular arrhythmia score during exercise testing. events per year;P<0.001) and improved the ventricular arrhythmia scores at the 3‐month (5 [range, 3–6] to 1.5
A 21-year-old woman presented to arrhythmia clinic with episodes of recurrent paroxysmal rapid palpitations. The patient had undergone an electrophysiology study and radiofrequency ablation elsewhere and was subsequently referred to our centre. What is the mechanism of the tachycardia?
Ventricular tachycardia (VT) ablation in structural heart disease improves arrhythmia free survival. Procedural factors that influence these outcomes are not well described.
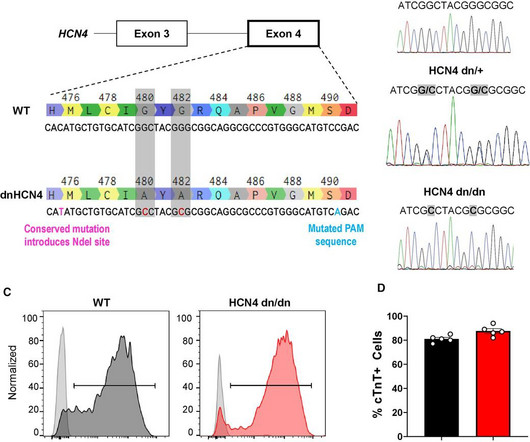
BackgroundHuman pluripotent stem cell-derived cardiomyocytes (hPSC-CMs) show tremendous promise for cardiac regeneration following myocardial infarction (MI), but their transplantation gives rise to transient ventricular tachycardia (VT) in large-animal MI models, representing a major hurdle to translation.
Atrial tachycardia (AT) originating from the left atrial appendage (LAA) is uncommon and the most difficult arrhythmia to eliminate. Therefore, we present the case of a 5-year-old girl with tachycardia-induced.
Volta Medical has announced it has entered into a Joint Development Agreement with GE Healthcare to enhance arrhythmia procedures with artificial intelligence (AI)-driven electrophysiology technologies. Our mission to combat complex heart rhythm diseases relies on optimizing interoperability.
A 15-year-old young male, presented to arrhythmia clinic with episodes of recurrent paroxysmal palpitations, lasting for several hours, requiring multiple admissions and DC cardioversion in the local hospital. What is the mechanism of the tachycardia? The 12 lead ECG (figure 1) and intracardiac recordings (figure 2) are shown below.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. Complex ventricular tachycardias involving the fascicular system (fascicular ventricular tachycardias [FVTs]) can be challenging. To summarize, 5 cases had prior ablation with 2 previously misdiagnosed as supraventricular tachycardia.
Studies have shown that mutations in the RYR2 gene, which encodes the RyR2 protein, are linked to several cardiac arrhythmias, including catecholaminergic polymorphic ventricular tachycardia (CPVT), long QT syndrome (LQTS), calcium release deficiency syndrome (CRDS), and atrial fibrillation (AF).
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. During early childhood, 50% of patients develop multifocal atrial tachycardia, a treatment-resistant tachyarrhythmia of unknown pathogenesis. BACKGROUND:GermlineHRASgain-of-function pathogenic variants cause Costello syndrome (CS).
IntroductionFocal atrial tachycardia (FAT) is predominant in the pediatric population. A 12-lead electrocardiogram revealed a narrow QRS complex tachycardia with a rate of 157 beats per minute and a prolonged RP relationship. Echocardiography indicated a severely reduced ejection fraction of 22%.
Abstract Introduction We report the case of an 18-year-old female with recurrent syncope that was discovered to have congenital long QT syndrome (LQTS) and episodes of a transiently short QT interval after spontaneous termination of polymorphic ventricular tachycardia.
In the past decade, major advances were made in catheter ablation for arrhythmias and implantation of cardiac implantable electronic devices.1 1 Catheter ablation for atrial fibrillation (AF) and ventricular tachycardia (VT) has become the standard of care for many patients presenting with these arrhythmias.2–4
Unlike paroxysmal AF, which describes symptoms that last for seven days or fewer, persistent AF is a sustained arrhythmia that lasts for more than a week 1. Early treatment of persistent AF can reduce the risk of blood clots, stroke, and heart failure, and may prevent the disease from becoming permanent.
An eager electrophysiology fellow was sitting next to his mentor, on the plane ride back from the American College of Cardiology Scientific Sessions, putting together slides on highlights of the meeting. The results of the Multicenter Unsustained Tachycardia Trial (MUSTT) were presented at the late breaking sessions.
Abstract Background The mechanism of typical slow-fast atrioventricular nodal re-entrant tachycardia (AVNRT) and its anatomical and electrophysiological circuit inside the right atrium (RA) and Koch's Triangle (KT) are not well known. The mean SR cycle length (CL) was 784.1 ± 6 ms and the mean tachycardia CL was 361.2 ± 54 ms.
Abstract Introduction Patients with viral myocarditis can present with challenging life-threatening arrhythmias. Catheter ablation can be a life-saving procedure in some patients with recurrent drug-refractory ventricular arrhythmias.
This measurement has been correlated with those made at electrophysiology study and may predict the potential risk of rapid anterograde conduction if the person develops atrial fibrillation. QT prolongation and the occurrence of ventricular arrhythmias with exercise are another important aspect of exercise testing in children.
Abstract Introduction Supraventricular tachycardia (SVT) is a common pediatric arrhythmia. Exclusion criteria were pre-excitation, ectopic atrial tachycardia, and hemodynamically significant heart disease. Beta blockers (BBs) and calcium channel blockers (CCBs) are used for treatment despite little data examining their use.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. BACKGROUND:Epicardial approach in ventricular tachycardia (VT) ablation is still regarded as a second-step strategy, due to the risk of complications.
ECG data during the clinical arrhythmia (ventricular tachycardia [VT], upper left figure) is analyzed with an artificial intelligence algorithm which identifies a probable location of the source of the arrhythmia (left ventricular anterolateral papillary muscle, lower left figure). Use of the system was associated with a 19.0%
Procedural data and electrophysiology (EP) laboratory times were systematically collected and analyzed. The primary endpoint was any AF or atrial tachycardia recurrence at 12 and 24 month follow up.Resultsthe study cohort was composed by 138 patients (mean age was 5911 years, 38% female) and successful PVI was achieved in 100% of cases.
We aimed to investigate the prevalence of NSVT in patients with ATTRwr-CA, and the association of NSVT with sustained ventricular arrhythmias (VA) and all-cause mortality.
A 37-year-old woman with biventricular repair for pulmonary atresia and an intact ventricular septum was referred for an electrophysiological study in the context of recurrent atrial arrhythmias with multiple electrical cardioversions. Her clinical tachycardia was easily inducible and had a cycle length (TCL) of 340 ms.
Patients with Brugada syndrome who are asymptomatic and have no ventricular tachycardia/ventricular fibrillation inducibility by programmed electrical stimulation are at extremely low risk of experiencing late life-threatening arrhythmias. Methods Patients with BrS ( n = 523; mean age, 51 ± 13 years; male, n = 497) were enrolled.
ABSTRACT Background Recent advancements in ultra-high-density mapping (UHDM) featuring automated functionalities have enhanced our understanding of micro-reentrant atrial tachycardias (mAT) circuits and the precise localization of the origin. Low voltage areas (<0.1mV) were detected in all mAT cases and colocalized with the origin site.
Although the QDOT MICRO™ Catheter was mainly designed for pulmonary vein isolation (PVI) its versatility to treat atrial fibrillation (AF) and other types of arrhythmias was recently evaluated by the FAST and FURIOUS study series and other studies and will be presented in this article.
Objective We report the feasibility, safety, and clinical efficacy of focal monopolar PFA in patients with the origin of their atrial arrhythmia in the SVC. Coronary vasospasm occurred (and quickly resolved after injection of nitroglycerin) in one patient during additional ablation of a focal atrial tachycardia at the coronary sinus ostium.
The advent of transseptal puncture has enabled the study of atrial fibrillation mechanisms, while epicardial access has enabled exploration of the epicardium in ventricular arrhythmias (ventricular tachycardia/ventricular fibrillation [VF]).1,2
Abstract Introduction Dual atrioventricular nodal non-reentrant tachycardia (DAVNNT) is a rare and challenging-to-diagnose arrhythmia, without previous reports associating it with a leftward inferior extension (LIE).
This can be a source of cardiac arrhythmia as well. An important cause of arrhythmias in Ebstein’s anomaly is the presence of a right sided accessory atrioventricular pathway or WPW syndrome. Electrophysiological study will show that, and this pathway can be ablated. This portion is known as atrialized right ventricle.
Case A 47-year-old male presented with atrial tachycardia 6 months post heart transplant. Electrophysiologic study demonstrated atrial fibrillation originating from native heart and propagated through atrio-atrial connections to the donor heart. This arrhythmia was successfully terminated with radiofrequency ablation.
ABSTRACT Introduction The aim of this study was to describe our experience and outcome of ablation therapy for arrhythmias in pediatrics at a tertiary care center. The data collected included type of arrhythmia, ablation technique, age and weight at ablation, procedure complications, medications used, and outcome assessment.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. Colchicine did not prevent atrial arrhythmia recurrence at 2 weeks (31% versus 32%; hazard ratio [HR], 0.98 [95% CI, 0.59–1.61];P=0.92) BACKGROUND:Inflammation may promote atrial fibrillation (AF) recurrence after catheter ablation. 2.02];P=0.89). 1.99];P=0.55).CONCLUSIONS:Colchicine
Abstract Introduction We report the case of a 37-year-old male athlete, who developed during exercise atrial and ventricular arrhythmias. Conclusions The findings in our patient may suggest some increased ventricular excitability using programmed ventricular stimulation in CASQ2 polymorphic ventricular tachycardia patients.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content