This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
UC San Diego Health is the first in San Diego to successfully implant the world’s first dual chamber and leadless pacemaker system to help treat people with abnormal heart rhythms. Holding the device and pictured above is Ulrika Birgersdotter-Green, MD, cardiologist and director of pacemaker and ICD services at UC San Diego Health.
A pacemaker modified for newborns' tiny bodies safely and effectively stabilized their heart rhythms for up to two years, according to new research published in Circulation: Arrhythmia and Electrophysiology.
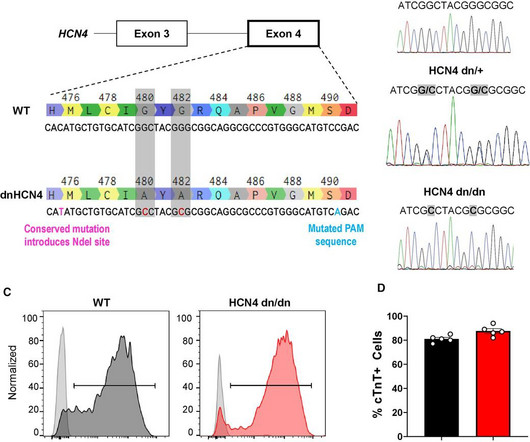
ConclusionsWhile genetic silencing of the pacemaker ion channel HCN4 suppresses the automaticity of hPSC-CMs in vitro, this intervention is insufficient to reduce VT risk post-transplantation in the pig MI model, implying more complex mechanism(s) are operational in vivo.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Seeing as the patient has a single chamber ICD/pacemaker, pacing the ventricle will also lead to AV dyssynchrony that will compromise ventricular filling, further impairing hemodynamics. small squares in width (260ms).
Written by Willy Frick A woman in her 90s with a history of end stage renal disease and complete heart block status post dual chamber pacemaker presented from home with acute onset dyspnea. As per Dr. Frick — pacemaker spikes are best seen in lead aVL of ECG #1. ECG is shown below. What do you think?
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. HCN inhibitors targeted pacemaker-like activity in mutant ACMs. Electrophysiological assessment revealed an increased number of pacemaker-like cells with elevated funny current densities among mutant ACMs.
While these are well tolerated by the young athlete, there is evidence that generally from the fifth decade of life onwards, such arrhythmias can degenerate into pathological symptomatic bradycardia requiring pacemaker therapy.
ABSTRACT Introduction Atrial fibrillation (AF) is the most common arrhythmia, and atrioventricular (AV) node ablation with pacemaker implantation is a therapeutic option for refractory cases. However, AV node ablation in patients with bioprosthetic tricuspid valves poses technical challenges.
ABSTRACT Introduction Use of implantable loop recorder (ILR) for the diagnosis and documentation of cardiac arrhythmia has gained popularity during the last decade. Although ILR RM transmissions have been shown to have significant false positive alerts, a true positive alert suggesting a wrong arrhythmia diagnosis has not been shown to date.
Massie Block -Ref 1) But, if there is something unusual in the clinical history, be ready to investigate until the arrhythmia, or at least the anxiety disappears. Clinical and electrophysiologic findings in patients with paroxysmal slowing of the sinus rate and apparent Mobitz type II atrioventricular block. Reference 1. PMID: 668079.
LBBAP significantly improved LVEF without causing fatal ventricular arrhythmias. All patients had a reduced LVEF of 36%–50% and underwent pacemaker implantation. No fatal ventricular arrhythmias occurred. Conclusion LBBAP significantly improved cardiac systolic dysfunction without causing fatal ventricular arrhythmias.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. BACKGROUND:The incidence and prognosis of right bundle branch block (RBBB) following transcatheter aortic valve replacement (TAVR) are unknown.
Arrhythmia-free survival at 1 year was 72.6%. However concomitant infections (pneumonia n =5/301 [1.7%], urinary-tract-infections n =4/301, [1.3%]) and pacemaker-implantation n =6/301 (2%) occurred more commonly. However, concomitant infections and pacemaker implantations occur in this cohort.
He received a permanent pacemaker during the subsequent inpatient stay. Chapter 17: Ventricular Arrhythmias. Josephson’s Clinical Cardiac Electrophysiology: Techniques and Interpretations (6th ed). The patient advised overall improvement with complete resolution of symptoms. Hospital transport was unremarkable. 2] Meyers, H.
Negative predictors of adverse outcome: Pacemaker Pre-syncope or "near-syncope," but there is still some small risk (5, 18) These last two are identified in studies, but I consider them dangerous signs and symptoms in their own right, as above: 10. The most recent and probably best study is this: Canadian Syncope Arrhythmia Risk Score.
So, we are looking for signs of an underlying regular atrial rhythm ( with perhaps slight sinus arrhythmia ) — and it is much easier to find this when you know what you are looking for! ( A permanent pacemaker was placed and the patient was atrial paced at 60bpm. After pacemaker placement — a ß-blocker was initiated.
How does a pacemaker accomplish RBBB morphology? Quick aside on device terminology (feel free to skip): A "single chamber" pacemaker is a device with only one lead. A "dual chamber" pacemaker is a device with an atrial lead and a ventricular lead. By ignoring this, the pacemaker reduces the likelihood of PMT.
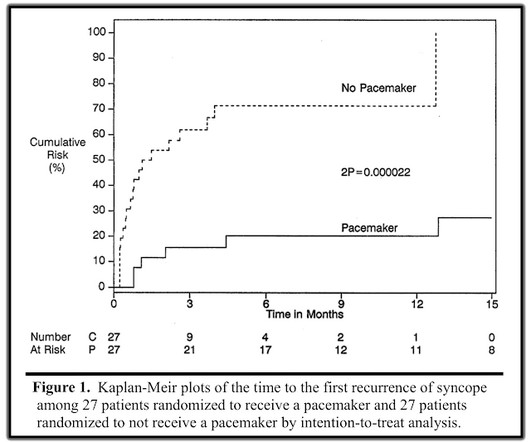
He was discharged with an event monitor and electrophysiology follow up. If the block is not vagal in nature, the patient should receive a pacemaker. There was a randomized trial to determine whether pacemakers could benefit patients with vasovagal syncope, aptly named The North American Vasovagal Pacemaker Study (VPS).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content