This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
EKG with paced complexes shown below shows much narrower QRS complex and echocardiogram showed improved LV systolic function primarily due to improvement in LV dyssynchrony. (J Even with tachycardia and a paced QRS duration of ~0.16 J Am Coll Cardiol.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Hopefully a repeat echocardiogram will be performed outpatient. The Initial ECG in Today's Case: As per Dr. Meyers — the initial ECG in today's case shows sinus tachycardia with bifascicular block ( = RBBB/LAHB ).
It's a very "fun" ECG, with initial ectopic atrial tachycardia (negative P waves in inferior leads conducting 1:1 with the QRSs), followed by spontaneous resolution to sinus rhythm. The emergent echocardiogram showed normal EF, no WMA, and normal valve function. What About the Tachycardia? Triage ECG: What do you think?
Here is her ED ECG: Here is the ED physician's interpretation: IMPRESSION UNCERTAIN REGULAR RHYTHM, wide complex tachycardia, likely p-waves. LEFT BUNDLE BRANCH BLOCK [120+ ms QRS DURATION, 80+ ms Q/S IN V1/V2, 85+ ms R IN I/aVL/V5/V6] Comparison Summary: LBBB and tachycardia are new. This is clearly ventricular tachycardia.
This can initiate ventricular arrhythmias like polymorphic ventricular tachycardia (PMVT). Transthoracic echocardiogram showed normal biventricular systolic function. Background:R-on-T phenomenon occurs when an electrical stimulus is delivered at a critical point during ventricular repolarization.
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. It is hard to make out P waves but you can see them best in V2, and notches in the T waves in other leads - this is a sinus tachycardia with a very long PR interval indicating first degree block.
There is sinus tachycardia. Sinus tachycardia, which exaggerates ST segments and implies that there is another pathology. I have always said that tachycardia should argue against acute MI unless there is cardiogenic shock or 2 simultaneous pathologies. Here is that ECG: What do you think? No wall motion abnormality.
Additionally, his cardiac telemetry monitor showed runs of accelerated idioventricular rhythm, a benign arrhythmia often associated with coronary reperfusion. Additionally, a bedside echocardiogram showed no wall motion abnormality and normal LV function. He had multiple episodes of bradycardia and nonsustained ventricular tachycardia.
We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. The differential of a regular narrow QRS tachycardia is sinus tachycardia, SVT, and atrial flutter with regular conduction. Now the patient is in sinus tachycardia. She had an echocardiogram which was normal.
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below. Learning points 1.
We believe they are likely a normal variant in this context, and the study above failed to identify any clinically significant finding after exam and echocardiogram in 110 children with bifid T waves. sec and voltage greater than or equal to 0.05 Note that the P-P interval between P waves “ b -to- c ” and “ d -to- e ” are not the same!
Notice there is tachycardia. I have warned in the past that one must think of other etiologies of ischemia when there is tachycardia. In this case, the patient had failed to take his atenolol in the AM and was having reflex tachycardia in addition to ACS. Seventh , an immediate echocardiogram can make the distinction.
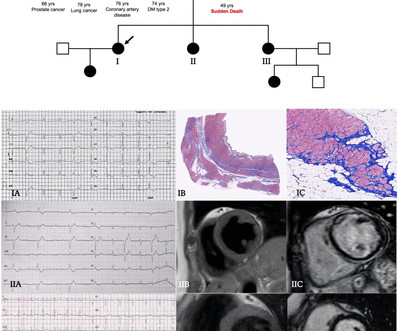
An echocardiogram was done. He has a family history concerning for arrhythmia. Given the circumstances of his car crash, we presume it was due to an underlying arrhythmia. He has a family history concerning for arrhythmia with his father requiring some sort of device (PPM, ICD, unclear) at a young age.
See this case: what do you think the echocardiogram shows in this case? Systematic Assessment of the ECG in Figure-1: My Descriptive Analysis of ECG findings in Figure-1 is as follows: Sinus tachycardia at ~110/minute. A slightly prolonged QTc ( although this is difficult to assess given the tachycardia ). A normal PR interval.
No arrhythmias occurred en route. Unfortunately there is no echocardiogram accessible because the patient checked himself out of the hospital in order to get back to his home state before it could be completed. C linically — the rhythm we see in the long lead II of ECG #3 behaves similar to MAT, even though there is no tachycardia.
A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity. myocardial infarction), arrhythmias, valvular pathology, shunts, or outflow obstructions. Aortic angiogram did not reveal aortic dissection.
Twenty-one (41%) had normal echocardiogram, 13 (25%) a hypokinetic non-dilated cardiomyopathy (HNDC) and 17 (33%) a dilated cardiomyopathy (DCM). Twenty-one (41%) had normal echocardiogram, 13 (25%) a hypokinetic non-dilated cardiomyopathy (HNDC) and 17 (33%) a dilated cardiomyopathy (DCM).
Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. Later, he underwent a formal echocardiogram: Very severe left ventricular enlargement (LVED diameter 7.4 An ECG was recorded: This shows a regular narrow complex tachycardia at a rate of about 160. C (99 °F), Resp (!)
However, an echocardiogram is a different test, also conducted for heart activity. Arrhythmia In simple words, arrhythmia refers to an irregular heartbeat. A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. ECG and EKG refer to the same thing.
We can see enough to make out that the rhythm is sinus tachycardia. Tachycardia is unusual for OMI, unless the patient is in cardiogenic shock (or getting close). A bedside ultrasound should be done to assess volume and other etiologies of tachycardia, but if no cause of type 2 MI is found, the cath lab should be activated NOW.
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD.
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. The most recent and probably best study is this: Canadian Syncope Arrhythmia Risk Score. Vasovagal syncope is generally benign.
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). The possibility of an ischemic cause of the ventricular arrhythmia has to be considered! A workup was undertaken in search of a cause of the patient's ventricular arrhythmia. No PVCs are seen.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content