This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The word arrhythmia comes from two Greek words. So arrhythmia literally means absence or loss of rhythm. A cardiac arrhythmia therefore means loss of cardiac rhythm. The first is ‘a-’ which means absence or loss and the second is ‘rhythmos’ which means rhythm. Most dysrhythmias once identified are easily treatable.
Arrhythmias (Irregular Heartbeats) Persistent abnormal heart rhythms can disrupt the heart’s pumping efficiency, eventually causing it to enlarge to maintain blood flow. Cardiac Arrest or Sudden Death: Cardiomegaly increases the risk of life-threatening arrhythmias, which can cause sudden cardiac arrest.
Regular check-ups allow your cardiologist to detect these issues through tests like blood work, EKGs, and echocardiograms. Family History: Regular check-ups are even more critical if you have a family history of heart disease. Your cardiologist can assess your risk factors and implement preventive measures.
The study’s findings, published in npj Digital Medicine , suggest AI could one day be employed to analyze images from a common imaging test called an echocardiogram, which uses sound waves to capture pictures of the heart. The team trained a program to study more than 100,000 echocardiogram videos from patients with atrial fibrillation.
He had his echocardiogram done already and was normal. Massie Block -Ref 1) But, if there is something unusual in the clinical history, be ready to investigate until the arrhythmia, or at least the anxiety disappears. I don’t know, whether a single blocked P could by any way a concealed Wenke -Bach. What does the guidelines say
It is also published in Heart Rhythm , the official journal of the HRS, Journal of Arrhythmia , the official journal of the APHRS, and Journal of Interventional Cardiac Electrophysiology , the official journal of the LAHRS. Antiarrhythmic drugs are advised for some patients to prevent arrhythmia recurrences early after the procedure.
Arrhythmias: Genetic mutations can also predispose individuals to irregular heart rhythms, such as atrial fibrillation or long QT syndrome, which may increase the risk of stroke or sudden cardiac arrest. Heart imaging, such as echocardiograms or CT scans. Key screenings include: Blood pressure and cholesterol checks.
During the intravenous lacosamide infusion, the patient developed sudden cardiac arrest caused by ventricular arrhythmias necessitating resuscitation. Workup including routine laboratory results, 12-lead electrocardiogram (ECG), echocardiogram, and coronary angiogram was non-specific.
EKG with paced complexes shown below shows much narrower QRS complex and echocardiogram showed improved LV systolic function primarily due to improvement in LV dyssynchrony. In this specific case, Left Bundle Branch (LBB) area pacing was pursued to achieve cardiac resynchronization.
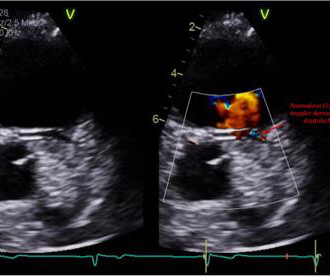
Electrocardiogram in clinic showed sinus arrhythmia with early repolarization and no ischemic changes. The echocardiogram showed normal cardiac structure and function, however, there was a concern for possible anomalous origin of the left coronary artery.
vs. 4.5%, p =0.96) on transesophageal echocardiogram did not differ. Both major (1.4% vs. 2.1%, p =0.72) and minor (27.8% vs. 19.4%, p =0.17) in-hospital complications were similar between the combined and control group, respectively. At 45 days, presence of peri-device leak (18.3% vs. 30.4%, p =0.07) and device related thrombosis (4.5%
Twenty-one (41%) had normal echocardiogram, 13 (25%) a hypokinetic non-dilated cardiomyopathy (HNDC) and 17 (33%) a dilated cardiomyopathy (DCM). Clinical contexts leading to diagnosis were SCD in 3 (6%), ventricular arrhythmias in 15 (29%), chest pain in 8 (15%), heart failure in 6 (12%) and familial screening in 20 (38%).
Hopefully a repeat echocardiogram will be performed outpatient. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). NOTE: Prediction of cardiac contusion "severity" on the basis of cardiac arrhythmias and ECG findings — is an imperfect science. No cardiac MRI was done.
The echocardiogram showed a normal EF without any abnormalities. The "good news" ( from an arrhythmia interpretation perspective ) — is that we now see P waves much better than we did in the initial ECG. That said, for readers with an interest in complex arrhythmias — Isn't this series of serial tracings fascinating! =
Echocardiogram showed LVEF 66% with normal wall motion and normal diastolic function. This is a critically important determination because of the 2017 AHA/ACC/HRS Guidelines for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death. Two subsequent troponins were down trending.
Additionally, his cardiac telemetry monitor showed runs of accelerated idioventricular rhythm, a benign arrhythmia often associated with coronary reperfusion. Additionally, a bedside echocardiogram showed no wall motion abnormality and normal LV function. Patient 2 was seen immediately after patient 1 by the same cardiologist.
ILRs detected various arrhythmias, with ventricular arrhythmias linked to spontaneous type 1 ECGs and fever. Bradyarrhythmias and atrial arrhythmias, common even in young patients, caused arrhythmic syncope in 60% of cases. ILRs may benefit BrS patients with unexplained syncope. Memorial Lecture for Dr. Alain Cribier: Prof.
Yes, COVID-19 symptoms can resemble a heart attack, including chest pain, shortness of breath, and changes in echocardiogram or EKG. Electrocardiograms (EKG or ECG): This diagnostic method effectively detects irregular heartbeats or arrhythmias by analyzing the electrical signals in the heart.
An echocardiogram showed severely reduced global systolic function with an EF of 20-25% and an LV apical thrombus. An echocardiogram showed an EF of 20-25%. At this point, there was no improvement in LV function and he was out of the convalescent phase of his MI, so the decision was made to install an ICD for arrhythmia prophylaxis.
However, an echocardiogram is a different test, also conducted for heart activity. Arrhythmia In simple words, arrhythmia refers to an irregular heartbeat. Electrocardiogram, echocardiogram, and some other tests are done for patients with cardiac arrest. ECG and EKG refer to the same thing.
Abstract Introduction Cavo-tricuspid isthmus (CTI) dependent atrial flutter (AFL) is one of the most common atrial arrhythmias involving the right atrium (RA) for which radiofrequency catheter ablation has been widely used as a therapy of choice. However, there is limited data on the effect of this intervention on cardiac size and function.
CS has a range of clinical syndromes: impaired conduction, arrhythmias, heart failure, and sudden cardiac death. An echocardiogram revealed normal biventricular function and morphology. It is characterized by a dysregulated T-cell driven immune response which generates non-necrotic inflammatory granulomas with myocardial infiltration.
WPW Cardiac arrhythmias ( including AFib ). Cardiac cath showed normal coronary arteries. Tall R wave in lead V1 and/or early transition in the chest leads ( reflecting increased "septal" forces ). Abnormal ST-T wave abnormalities. Conduction defects (ie, LBBB, IVCD ). The Problem: None of the above ECG findings are specific for HCM.
This can initiate ventricular arrhythmias like polymorphic ventricular tachycardia (PMVT). Transthoracic echocardiogram showed normal biventricular systolic function. Circulation, Volume 150, Issue Suppl_1 , Page A4143264-A4143264, November 12, 2024. Her electrolytes and cardiac enzymes were unremarkable.
The diagnosis was a bit hard to find in the chart, and the echocardiogram did only stated "assymetric hypertrophy." I added, "Makes me wonder if this could be myocarditis in a younger adult — maybe even with sinus arrhythmia." It turns out that she has hypertrophic cardiomyopathy. Figure-1: The initial ECG in today's case.
We believe they are likely a normal variant in this context, and the study above failed to identify any clinically significant finding after exam and echocardiogram in 110 children with bifid T waves. sec and voltage greater than or equal to 0.05 Note that the P-P interval between P waves “ b -to- c ” and “ d -to- e ” are not the same!
Echocardiogram is indicated (Correct) C. Start aspirin and Plavix Correct answer: (B) (B) Echocardiogram is indicated. Which of the following is the best statement to describe further clinical management? No further workup is indicated B. Start furosemide for diuresis D. Start with a Free Trial.
An echocardiogram was done. He has a family history concerning for arrhythmia. Given the circumstances of his car crash, we presume it was due to an underlying arrhythmia. He has a family history concerning for arrhythmia with his father requiring some sort of device (PPM, ICD, unclear) at a young age.
Formal echocardiogram showed normal EF, no wall motion abnormalities, no pericardial effusion. Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7]. Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias. No more troponins were done.
The emergent echocardiogram showed normal EF, no WMA, and normal valve function. MY point that is relevant to optimal arrhythmia interpretation — is to always look to see if there is a "break" in the rhythm at the onset or offset of the tachycardia — since if present, this will often tell you the specific diagnosis!
Angina is another common symptom due the hypertrophy which causes a coronary supply demand mismatch Symptoms of HCM include syncope/near syncope, which could be precipitated by exertion, hypovolemia, rapid standing, Valsalva manoeuvre, diuretics, vasodilators or arrhythmia. Palpitations can be felt if there are arrhythmias.
The patient underwent an emergent formal echocardiogram to look for wall motion abnormality: The estimated left ventricular ejection fraction is 63 %. Exclusion criteria were age less than 18, SBP less than 100 mmHg, echocardiogram with EF less than 50%, STEMI, pregnancy, and trauma. No wall motion abnormality.
While awaiting transfer to the cath lab, STAT echocardiogram was performed and showed LVEF 30-35%, as well as anterior, inferior, and apical hypokinesis, and apical thrombus. Jenkins and Frick — I offer 3 additional examples of artifactual distortion ( excerpted from my ECG Blog ) — that resulted in arrhythmia misdiagnosis.
A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7]. There was a 0.9% per year incidence of SCD in this cohort [1].
This transformation extends to the use of machine learning (ML) algorithms developed by startups, which analyze medical imaging data such as ECGs, echocardiograms, and cardiac MRI scans. These algorithms, trained on large datasets, recognize patterns and features associated with heart diseases.
Due to limitations of echocardiogram in evaluating the right ventricle, magnetic resonance imaging study of the right ventricle along with that of the left ventricle has been reported. Effect of exercise on right ventricle. Twenty-one male endurance athletes were compared with untrained control subjects.
Seventh , an immediate echocardiogram can make the distinction. Sixth , placement of posterior leads (take leads V4-V6 and place them at the level of the tip of the scapula, with V4 placed at the posterior axillary line ("V7"), V6 at paraspinal area ("V9"), and V5 ("V8") between them. At lease 0.5
Here is the post PCI EKG: And a few hours after that: The post PCI echocardiogram showed: Normal estimated left ventricular ejection fraction, 57%. The rhythm in Figure-1 is sinus bradycardia and arrhythmia. This is a large OMI that has Zero ST Elevation but can be diagnosed by ECG features other than ST Elevation!!
She had an echocardiogram which was normal. Even experienced providers make the mistake of using the term, “SVT” as a specific diagnosis — when in fact this generic term includes all arrhythmias in which the rate is “tachycardic” ( ie, ≥100 in an adult ). This includes sinus tachycardia, atrial fibrillation or flutter, MAT, and others.
Echocardiogram: Estimated left ventricular ejection fraction, lower limits of normal; 45-50%. There are 6 KEY parameters to consider in systematic assessment of any arrhythmia. Tele Monitor: Normal sinus rhythm throughout, no ectopic atrial or ventricular beats. Regional wall motion abnormality-inferior/inferoseptum: akinetic.
No arrhythmias occurred en route. Unfortunately there is no echocardiogram accessible because the patient checked himself out of the hospital in order to get back to his home state before it could be completed. He was expected to arrive at the tertiary care center within 60 minutes of the call. To our knowledge, the patient did well.
I have ordered an echocardiogram which will be done today, after that patient can be discharged to home with follow-up in 2 to 3 months." NOTE #3: In the context of a long QTc or ischemia — the finding of ST segment and/or T wave alternans may predict the occurrence of malignant ventricular arrhythmias. The echo was normal.
See this case: what do you think the echocardiogram shows in this case? POCUS showed good LV-function and no pericardial effusion. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. The patient had mild but diffuse abdominal tenderness.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content