This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Coronary artery spasm (CAS), or Prinzmetal angina, is a recognised cause of myocardial ischaemia in non-obstructed coronary arteries which typically presents with anginal chestpain. The patient presented with recurrent palpitations and pre-syncope, with no chestpain.
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chestpain. He was eating lunch when he had sudden onset chest pressure, 9/10, radiating to his back, with sweating and numbness in both hands.
This was written by Magnus Nossen, from Norway, with comments and additions by Smith A 50 something smoker with no previous medical hx contacted EMS due to acute onset chestpain. Upon EMS arrival the patient appeared acutely ill and complained of chestpain. An ECG was recorded immediately and is shown below.
Cingolani, director of Cardiogenetics and Preclinical Research in the Department of Cardiology in the Smidt Heart Institute at Cedars-Sinai, is exploring new ways to help patients with ventricular tachycardia (VT), a recurring, abnormally fast and irregular heartbeat that starts in the lower chambers, or ventricles, of the heart.
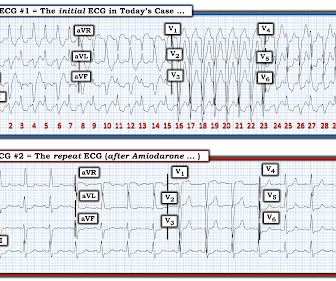
A prehospital 12-lead was recorded: There is a regular wide complex tachycardia. The computer diagnosed this as Ventricular Tachycardia. There is a wide complex regular tachycardia at a rate of 226. Toothache, incidental Wide Complex Tachycardia Could it be fascicular VT or Bundle Branch VT ( i.e., idiopathic VT )?
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. There is sinus tachycardia. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. Sinus tachycardia, which exaggerates ST segments and implies that there is another pathology.
Shortly after receiving epinephrine, the patient developed new leg cramps and chestpain. The chestpain was described as sharp and radiated to both arms. During active chestpain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. She presented to the emergency department after a couple of days of chest discomfort. Answer : The ECG above shows a regular wide complex tachycardia. Cardiac output (CO) was being maintained by the tachycardia.
In the evening, a middle-aged man complained of chestpain at the nursing home. His chestpain was vague. He mentioned "cancer" and "chest". He mentioned "cancer" and "chest". There is a narrow complex tachycardia at a rate of 130. I’ll focus my comments on arrhythmia diagnosis. Is is sinus?
Just as important is pretest probability: did the patient report chestpain prior to collapse? Confirmation of sinus tachycardia should be easy to verify when the heart rate slows a little bit ( as the patient's condition improves ) — allowing clearer definition between the T and P waves. Then assume there is ACS.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
Note the Timed Contents that I detail below facilitate finding specific material. == ECG Podcast #4 — All About Comparison ECGs for 12-Leads and Arrhythmias ( Comparing ECGs seems so "easy" to do — but so often is not done correctly! ) — published by Mayo Clinic CV Podcast Series on 5/21/2024 ( 35 minutes ). What are the problems?
Chest trauma was suspected on initial exam. The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma? He was intubated for altered mental status.
His previous echo one month prior shows the same thing: “consistent with old infarct in LAD vascular territory, with EF 45%” "I think there is something else causing his tachycardia which is exaggerating his EKG findings and mimicking an acute myocardial infarction." The patient spontaneously converted back to sinus tachycardia.
This 60-something with h/o COPD and HFrEF (EF 25%) presented with SOB and chestpain. Multifocal Atrial Tachycardia 2. Failure to follow this advice will undoubtedly lead to overlooking subtle acute MIs — and , it will especially lead to misdiagnosing many cardiac arrhythmias ( as was done in this case ). GET a 12-lead!
22:25 — What if you have a regular SVT ( = narrow-complex tachycardia ) without obvious P waves? ( And regarding arrhythmias: For more on the regular WCT — See My Comment in the May 5, 2020 post and in the April 15, 2020 post in Dr. Smith's ECG Blog. 11:35 — My views on: Will the computer ever be able to interpret complex arrhythmias?
Here is her ED ECG: Here is the ED physician's interpretation: IMPRESSION UNCERTAIN REGULAR RHYTHM, wide complex tachycardia, likely p-waves. LEFT BUNDLE BRANCH BLOCK [120+ ms QRS DURATION, 80+ ms Q/S IN V1/V2, 85+ ms R IN I/aVL/V5/V6] Comparison Summary: LBBB and tachycardia are new. This is clearly ventricular tachycardia.
This is the prehospital ECG from an 81 year old man with acute chestpain. Arrhythmia? Today’s case recalled that scenario for me, in that it features recognition of an arrhythmia that fooled ED staff into thinking the ECG was showing an acute infarction. The medics did NOT activate the cath lab. Would you give lytics?
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. Colchicine did not prevent atrial arrhythmia recurrence at 2 weeks (31% versus 32%; hazard ratio [HR], 0.98 [95% CI, 0.59–1.61];P=0.92) Postablation chestpain consistent with pericarditis was reduced with colchicine (4% versus 15%; HR, 0.26 [95% CI, 0.09–0.77];P=0.02)
A 90 yo with a history of orthostatic hypotension had a near syncopal event followed by chestpain. Chestpain was resolved upon arrival in the ED. Idioventricular rhythm is a common "reperfusion arrhythmia." Exactly how they relate to ischemia, chestpain, and reperfusion can only be speculated about.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. Patient 2 was seen immediately after patient 1 by the same cardiologist.
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Sinus tachycardia does not go this fast. A 60-something ow healthy male had syncope while on treadmill. What do you want to do?
The presenting complaint was chestpain — and the patient collapsed soon after arrival in the ED. The finding of a fairly regular, wide tachycardia without clear sign of atrial activity ( especially when seen in an acutely symptomatic patient ) — should immediately prompt a diagnosis of VT until proven otherwise.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
The ECG in Figure-1 was obtained from an older woman — who presented with chestpain and palpitations over the previous hour. This familial cardiac arrhythmia is the result of gene mutation. These patients are at high risk for malignant arrhythmias. BP = 140/90 mm Hg in association with the rhythm in Figure-1.
No chestpain. Figure-1: The initial ECG in today's case — obtained from an 86-year old man with presyncope, but no chestpain. ( L ADDERGRAM I llustration : Clarification of the mechanism in today's arrhythmia is best explained by laddergram illustration ( Figure-5 ). How would YOU interpret the ECG in Figure-1 ?
She reports that she is now unable to vagal out of her palpitations and is having shortness of breath and dull chestpain. We see a regular tachycardia with a narrow QRS complex and no evidence of OMI or subendocardial ischemia. Now the patient is in sinus tachycardia. Sinus tachycardia, AFlutter and ATach do not do this.
This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute. ie, with syncope-presyncope, fatigue, dyspnea, chestpain? ). 2 short runs of SVT ( presumably atrial tachycardia ).
He has a family history concerning for arrhythmia. Given the circumstances of his car crash, we presume it was due to an underlying arrhythmia. He has a family history concerning for arrhythmia with his father requiring some sort of device (PPM, ICD, unclear) at a young age. ST depression. Myocardial Contusion?
This should result in at least some positivity of QRS complexes as one moves toward the lateral chest leads. The finding of all negative QRS complexes in leads V3-thru- V6 therefore strongly suggests that the arrhythmia-associated impulse is not traveling over an AP ( Steurer et al — Clin. Cardiol 17:306-308, 1994 ).
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. A slightly prolonged QTc ( although this is difficult to assess given the tachycardia ).
A recent similar case: A 40-something with chestpain. Therefore, she underwent temporary pacemaker placement and overdrive pacing at a rate of 90 bpm to keep the heart rate up in order to prevent these PVCs triggering ventricular arrhythmia. Is this inferior MI? There is a bigeminy with very Bizarre looking PVCs.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. There are three mechanisms of arrhythmia: automatic, re-entry, and triggered.
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia. MY Thoughts on the ECG in Figure-1: The rhythm in ECG #1 — is sinus tachycardia at ~125/minute.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. myocardial infarction), arrhythmias, valvular pathology, shunts, or outflow obstructions. The patient’s mental status was altered and his skin was pale and dusky.
There was no chestpain. Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. VT is the second most common presenting arrhythmia. Vaso or inotropic medications are not harmless, and can precipitate life threatening arrhythmias. She had no known heart condition.
She denied chestpain and denied feeling any palpitations, even during her triage ECG: What do you think? She was awake, alert, well perfused, with normal mental status and overall unremarkable physical exam except for a regular tachycardia, possible rales at both bases, some mild RUQ abdominal tenderness.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. We can see enough to make out that the rhythm is sinus tachycardia. It was not worse with exertion or relieved by rest.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. However, he suddenly developed a series of malignant ventricular arrhythmias.
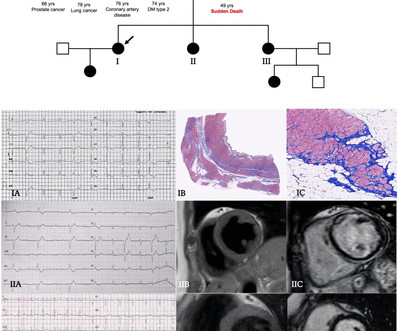
Clinical contexts leading to diagnosis were SCD in 3 (6%), ventricular arrhythmias in 15 (29%), chestpain in 8 (15%), heart failure in 6 (12%) and familial screening in 20 (38%). Significant right ventricular involvement was an exclusion criterion.
He did not have chestpain. ECG is consistent with severe hypokalemia and/or hypomagnesemia causing prolonged QT (QU) at high risk of Torsades (which is polymorphic ventricular tachycardia in the setting of a long QT interval). Chestpain in high risk patient. Here is his triage ECG: What do you think? Is it STEMI?
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The history in today's case with sudden loss of consciousness followed by chestpain is very suggestive of ACS and type I ischemia as the cause of the ECG changes. What do you think?
All of the patients presented with chestpain , and they are all in triage. I completely agree with Dr. Nossen that in this patient with new CP and sinus tachycardia with LAHB — that the T waves in each of the inferior leads are hyperacute ( ie, clearly disproportionately "bulky" given size of the QRS in these leads ).
This middle-aged man with no cardiac history but with significant history of methamphetamin and alcohol use presented with chestpain and SOB, worsening over days, with orthopnea. Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. BP:143/99, Pulse 109, Temp 37.2 °C
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content