This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
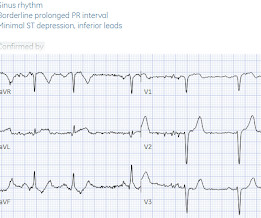
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. There are three mechanisms of arrhythmia: automatic, re-entry, and triggered.
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chestpain. He was eating lunch when he had sudden onset chest pressure, 9/10, radiating to his back, with sweating and numbness in both hands.
Written by Jesse McLaren A previously healthy 60 year old developed exertional chestpain with diaphoresis, and called EMS. There’s sinus arrhythmia with normal conduction, normal axis and normal voltages. Both reinforce the false STEMI/non-STEMI dichotomy, and are barriers to shifting towards the OMI paradigm.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0.
Click here to sign up for Queen of Hearts Access Case A 58-year-old woman presented to the ED with burning chestpain that started 2-3 hours earlier while sitting on a porch swing. See this post: Septal STEMI with ST elevation in V1 and V4R, and reciprocal ST depression in V5, V6. Also seen in inferior + RV OMI.)
Case sent by Logan Stark MD, written by Pendell Meyers A woman in her 70s presented with acute chestpain. Or perhaps the group beating is simply the result of sinus arrhythmia that by chance results in alternating R-R intervals of very similar size? No prior ECG was available. Here is her triage ECG: What do you think?
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. Inclusion criteria were chestpain, at least 2 serial cTnI in 24 hours, sinus rhythm , and at least 1 ECG.
A previously healthy middle-aged male presented shortly after the acute onset of chestpain very shortly before calling 911. On arrival, he was pain free: What do you think? Jerry Jones commented: "Any ST depression on the ECG of a patient with chestpain credible for ACS represents a reciprocal change until proved otherwise."
The patient presented with chestpain. If it is STEMI, it would have to be RBBB with STEMI. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. This ECG was sent from South Asia.
Shortly after receiving epinephrine, the patient developed new leg cramps and chestpain. The chestpain was described as sharp and radiated to both arms. During active chestpain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF.
The computer called it a normal ECG Algorithm unknown Aside : [There is some "sinus arrhythmia", which is indeed a normal finding. Sinus arrhythmia is sinus rhythm whose rate varies with respiration. If the longest P-P interval is 120 ms greater than the shortest, it is sinus arrhythmia. Burning pain subxiphoid and into throat."
There is clearly sufficient STE for STEMI criteria in leads V2 and aVL, but lead I has less than 1.0 mm of STE - thus, technically this ECG does not meet STEMI criteria, although it is a quite obvious OMI. This ECG was immediatel y discussed with the on-call cardiologist who said the ECG was "concerning but not a STEMI."
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
It is from a 50-something with chestpain: What do you think? This was marked as "Not a STEMI" by the physicians. It is not a STEMI, but it is diagnostic of an LAD OMI (Occlusion MI). In my opinion — AI is not yet "there" with regard to interpretation of complex cardiac arrhythmias. This was sent to me by a friend.
Written by Jesse McLaren, with edits from Smith and Grauer A 60 year old with no past medical history presented with two hours of chestpain radiating to the left arm, with normal vitals. But it doesn’t meet STEMI criteria, and was not identified by the computer or the over-reading cardiologist. What do you think?
The patient has acute chestpain. Any objective, rule-based analysis of this ECG would scream "STEMI" or "OMI". And I recognized this as a STEMI mimic. Instead — my thoughts were as follows: The rhythm is sinus , with marked bradycardia and a component of sinus arrhythmia. This was texted to me in real time.
Written by Pendell Meyers A woman in her 50s presented with acute chestpain and lightheadedness since the past several hours. It does not meet STEMI criteria. Luckily, 45 minutes later, with ongoing pain and a troponin I that resulted at 136 ng/L, the ECG was repeated: What do you think now? Anyway, she does say OMI.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He wrote most of it and I (Smith) edited.
Note the Timed Contents that I detail below facilitate finding specific material. == ECG Podcast #4 — All About Comparison ECGs for 12-Leads and Arrhythmias ( Comparing ECGs seems so "easy" to do — but so often is not done correctly! ) — published by Mayo Clinic CV Podcast Series on 5/21/2024 ( 35 minutes ). What are the problems?
Just as important is pretest probability: did the patient report chestpain prior to collapse? Cardiac arrest #3: ST depression, Is it STEMI? After cardiac arrest, I ALWAYS wait 15 minutes after an ECG like this and record another. The ST depression usually resolves, or is clearly resolving (getting much better).
A late middle-aged man presented with one hour of chestpain. Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? IV administration of potassium is indicated when arrhythmias are present or hypokalemia is severe (potassium level of less than 2.5
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7].
This can only be due to STEMI. My THOUGHTS on ECG #1: We are told that the patient in today’s case had an episode of severe chestpain 3 nights prior to admission. However, cardiogenic shock usually takes some time to develop, so it is probably subacute." Then I was told that the troponin I returned at greater than 50,000 ng/L.
And regarding arrhythmias: For more on the regular WCT — See My Comment in the May 5, 2020 post and in the April 15, 2020 post in Dr. Smith's ECG Blog. 2:25 — Dr. Grauer: The 1st Error : Too many clinicians in 2024 are still stuck in the outdated millimeter-based STEMI Paradigm”. 27:00 — SUMMARY by Dr. Anthony Kashou.
A 90 yo with a history of orthostatic hypotension had a near syncopal event followed by chestpain. Chestpain was resolved upon arrival in the ED. Idioventricular rhythm is a common "reperfusion arrhythmia." Exactly how they relate to ischemia, chestpain, and reperfusion can only be speculated about.
The presenting complaint was chestpain — and the patient collapsed soon after arrival in the ED. Looking at the location of ST elevation ( ie, in the inferior leads — and in V4,5,6 ) — and the location of ST depression ( ie, in leads I,aVL; V1,V2 ) — this ECG picture suggests an ongoing acute infero - postero - lateral STEMI.
This includes sinus arrhythmia — in which there is often slight variation in the P-P interval. This slight variation in sinus P wave regularity tends to be greater when a 2nd- or 3rd-degree AV block is present ( called ventriculophasic sinus arrhythmia — as shown in ECG Blog #344 ). For clarity — I have done this in Figure-4.
He did not have chestpain. Is it STEMI? Chestpain in high risk patient. A man in his 60s with a history of severe alcohol use disorder and epidural abscess on long-term ciprofloxacin presented to the emergency department after an episode of syncope while standing in line at a grocery store. What is going on here?
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
Later, I found old ECGs: 5 month prior in clinic: V5 and V6 look like OMI 9 months prior in clinic with no chest symptoms: V5 and V6 look like OMI 1 year prior in the ED with chestpain: V5 and V6 sure look like a STEMI For this ECG and chestpain in the ED, the Cath lab activated. There was no OMI.
The ECG in Figure-1 was obtained from a previously healthy older man — who complained of chestpain and “lightheadedness” while this tracing was recorded. His chestpain had begun the night before. Figure-1: 12-lead ECG and long lead II rhythm strip — obtained from an older man with chestpain and “lightheadedness. (
A 40-something male presented with dyspnea and left arm numbness, and perhaps some chest tightness, for 1 1/2 hours. This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. In any case, sinus arrhythmia is much less marked in ECG #2 after SL NTG with improvement of symptoms. Thelin et al.
If you saw this ECG only knowing that it is an acute chestpain patient, what would be your interpretation? However, in the context of the first ECG and the waning chestpain, this is diagnostic of reperfusion. Due to the severity of the pain and the high BP, they obtained an aortic dissection CT.
So this is a typical Brugada syndrome ECG, which can be easily mistaken for an acute myocardial infarction with ST elevation in anterior leads may be taken as STEMI if the person presents with chestpain for some other reason. An interesting fact is that many of the persons experience arrhythmias in Brugada syndrome with fever.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
In fact, there was no chestpain either. If you were thinking that this is not anterior OMI because there is no reciprocal ST depression , it is important to remember that half of anterior STEMI do NOT have any reciprocal ST depression. BUT look at the very prominent J-waves (J point notching)!! It is several mm high!
A 40-something woman had sudden chestpain. This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI.
They also documented "Reproducible chest tenderness." The patient said his chestpain was 4/10, down from 8/10 on presentation. Additional findings: No ST elevation." Remember that patients with OMI can have normal ECGs! Repeat hsTnI was 183 ng/L, up from 26 ng/L. Around noon, cardiology was called for evaluation.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. It was from a patient with chestpain: Note the obvious Brugada pattern. Bicarb 20, Lactate 4.2,
This ECG clearly meets STEMI criteria by the way, regardless of age or gender. This is a high troponin (most STEMI are above 10 ng/mL for troponin I). MY THOUGHTS on ECG #1 ( if it was the Only Tracing I Had ): There is sinus arrhythmia ( variable R-R interval — but all p waves conducting with a constant PR interval ).
This should result in at least some positivity of QRS complexes as one moves toward the lateral chest leads. The finding of all negative QRS complexes in leads V3-thru- V6 therefore strongly suggests that the arrhythmia-associated impulse is not traveling over an AP ( Steurer et al — Clin. Cardiol 17:306-308, 1994 ).
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. What do you see?
Dyspnea, Right Bundle Branch block, and ST elevation Here are two more cases where the differential diagnosis is acute OMI vs. LV aneurysm: Is this acute STEMI? 9 Hours of ChestPain and Deep Q-waves: Is it too late for Thrombolytics? LV Aneurysm? Would you give Thrombolytics?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content