This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. PR depression, which suggests pericarditis 4. Here is that ECG: What do you think? There is sinus tachycardia.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. Altogether, this strongly suggests inferolateral OMI, particularly in a patient with acute chestpain.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. Colchicine did not prevent atrial arrhythmia recurrence at 2 weeks (31% versus 32%; hazard ratio [HR], 0.98 [95% CI, 0.59–1.61];P=0.92) Postablation chestpain consistent with pericarditis was reduced with colchicine (4% versus 15%; HR, 0.26 [95% CI, 0.09–0.77];P=0.02)
In fact, there was no chestpain either. Pericarditis? If you were thinking that this is pericarditis, that would be possible in the absence of any clinical information. However, there is zero PR depression which would be VERY unusual in pericarditis. P.S.: Acute pericarditis may produce diffuse ST elevation.
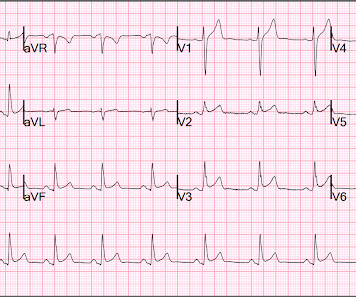
No chestpain. In a previously healthy adolescent ( who is 15 years old in today's case ) — the presentation of an acute febrile illness that is without a complaint of chestpain, is highly unlikely to be due to an acute MI. He was hemodynamically stable. How would YOU interpret the ECG in Figure-1 ?
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ).
All of the patients presented with chestpain , and they are all in triage. Triage is backed up, and 10 minutes into your shift one of the ED nurses brings your several ECG s that has not been overread by a physician. Which, if any, of these patients has OMI, with myocardium at risk and need for emergent PCI?
Haven't you been taught that this favors pericarditis? Weren't you taught that concave morphology favors pericarditis? Expert ECG interpretation can often distinguish normal variant STE from OMI from pericarditis. There is now a regular sinus rhythm ( there had previously been a fairly marked sinus arrhythmia in ECG #1 ).
He has a family history concerning for arrhythmia. Given the circumstances of his car crash, we presume it was due to an underlying arrhythmia. He has a family history concerning for arrhythmia with his father requiring some sort of device (PPM, ICD, unclear) at a young age. ST depression. Myocardial Contusion?
Given her reported chestpain, shortness of breath, and syncope, an ECG was quickly obtained: What do you think? The second most common cause of medical cardiac tamponade is acute idiopathic pericarditis. Both ST segment and T wave alternans have been known to precede malignant ventricular arrhythmias.
Patient 2 : 55 year old with 5 hours of chestpain radiating to the shoulder, with nausea and shortness of breath ECG: sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. This was missed by the treating physician, but the chestpain resolved with aspirin.
He was concerned because he had chestpain after his first mRNA vaccine and was uncomfortable with the risks of a second mRNA dose. He subsequently describes having sharp chestpain over the next few weeks. The pain resolved a few weeks later. He emphatically denies any history of cardiopulmonary disease.
days of chestpain that started as substernal and crushing in nature awakening him from sleep and occasionally traveling to right side of neck. The pain was described as constant, worse with deep inspiration and physical activity, sometimes sharp. My Thoughts on the ECG in Figure-1: The rhythm in ECG #1 is sinus arrhythmia.
A 26 year old male presented with syncope and chestpain. No signs of OMI" The chestpain resolved after some time, and another ECG was recorded: The ST Elevation is nearly gone. Syncope was sudden and without prodrome, and resulted in head trauma with a scalp laceration. Smith : I recognize this as a STEMI mimic.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content