This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. There are three mechanisms of arrhythmia: automatic, re-entry, and triggered.
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. The fact that R waves 2 through 6 are junctional does make ischemia more difficult to interpret -- but not impossible.
Click here to sign up for Queen of Hearts Access Case A 58-year-old woman presented to the ED with burning chestpain that started 2-3 hours earlier while sitting on a porch swing. V1 sits over both the RV and the septum, so transmural ischemia of either one with give OMI pattern in V1 and reciprocal STD in V5 and V6.
This was interpreted by the treating clinicians as not showing any evidence of ischemia. He did not remember whether he had experienced any chestpain. He was intubated in the field and sedated upon arrival at the hospital. Here is his presenting ECG: ECG 1, t = 0 What do you think? He was admitted to cardiology.
I went to the patient's chart: Elderly woman with stuttering chestpain and SOB, and dizziness. The unique " shape " of the prominent ST-T wave abnormalities in this tracing — that are much more suggestive of some significant form of LVH ( L eft V entricular H ypertophy ) rather than ischemia. What do you think now?
Shortly after receiving epinephrine, the patient developed new leg cramps and chestpain. The chestpain was described as sharp and radiated to both arms. During active chestpain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF.
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. The ECG does not show any definite signs of ischemia. The below ECG was recorded.
Written by Pendell Meyers A woman in her 50s presented with acute chestpain and lightheadedness since the past several hours. The STD maximal in V1-V4 is diagnostic of acute transmural posterior wall ischemia, most likely due to posterior OMI. Subendocardial ischemia does not localize. AI can do it too.
The ECG shows severe ischemia, possibly posterior OMI. But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. It takes time for that ischemia to resolve. Just as important is pretest probability: did the patient report chestpain prior to collapse?
A previously healthy middle-aged male presented shortly after the acute onset of chestpain very shortly before calling 911. On arrival, he was pain free: What do you think? Jerry Jones commented: "Any ST depression on the ECG of a patient with chestpain credible for ACS represents a reciprocal change until proved otherwise."
The patient presented with chestpain. Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada.
The computer called it a normal ECG Algorithm unknown Aside : [There is some "sinus arrhythmia", which is indeed a normal finding. Sinus arrhythmia is sinus rhythm whose rate varies with respiration. If the longest P-P interval is 120 ms greater than the shortest, it is sinus arrhythmia. Burning pain subxiphoid and into throat."
Written by Jesse McLaren, with edits from Smith and Grauer A 60 year old with no past medical history presented with two hours of chestpain radiating to the left arm, with normal vitals. 2] Conduction through the accessory pathway can be intermittent (with different degrees of pre-excitation), and affected by ischemia.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. However, he suddenly developed a series of malignant ventricular arrhythmias.
The patient has acute chestpain. Here was my answer: "Not ischemia. Instead — my thoughts were as follows: The rhythm is sinus , with marked bradycardia and a component of sinus arrhythmia. Tall R wave in lead V1 and/or early transition in the chest leads ( reflecting increased "septal" forces ).
He did not have chestpain. A prior ECG was available for comparison: Normal One might be tempted to interpret the ST depression as ischemia, but as Smith says, "when the QT is impossibly long, think of hypokalemia and a U-wave rather than T-wave." Chestpain in high risk patient. Is it STEMI?
She was hemodynamically stable — and did not have chestpain, lightheadedness or syncope. With P waves labeled — Isn't it now much easier to appreciate that the atrial rhythm is quite regular ( with no more than a slight sinus arrhythmia )? For those with a special interest in cardiac arrhythmias — READ ON! —
A 90 yo with a history of orthostatic hypotension had a near syncopal event followed by chestpain. Chestpain was resolved upon arrival in the ED. Is there ischemia? Idioventricular rhythm is a common "reperfusion arrhythmia." His previous ECG was normal. What is it? Answer below. But it is not conclusive.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The arrhythmia spontaneously converted before defibrillation was achieved. What do you think? What do you think?
In the evening, a middle-aged man complained of chestpain at the nursing home. His chestpain was vague. He mentioned "cancer" and "chest". I’ll focus my comments on arrhythmia diagnosis. P EARL # 2 : In my experience — the most commonly overlooked arrhythmia ( by far! ) Fluids were started.
This is ischemia until proven otherwise. A fixed stenosis in that other artery, especially in the context of hypotension from the occlusion of the first coronary artery, can lead to ischemia and very poor LV function and worsening shock. I learned that the patient is on Sotalol for control of PVCs. This explains the long QT.
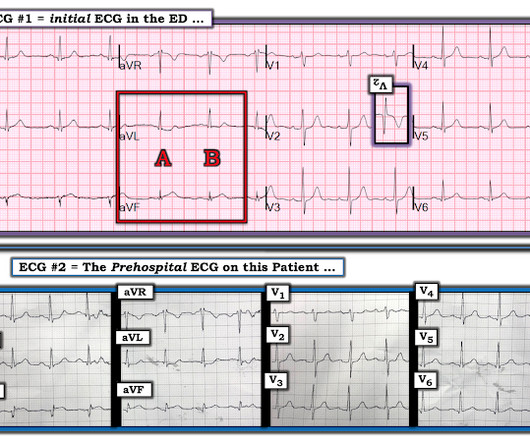
My written interpretation on a tracing such as this one would read, "Marked LVH and 'strain' and/or ischemia — with need for clinical correlation." BOTTOM Line: Today's patient presented with a 2-3 day history of chestpain and the ECG shown in Figure-1. WPW Cardiac arrhythmias ( including AFib ).
This may result in ischemia (lack of oxygen to the heart muscle), causing parts of the heart to weaken and enlarge. Arrhythmias (Irregular Heartbeats) Persistent abnormal heart rhythms can disrupt the heart’s pumping efficiency, eventually causing it to enlarge to maintain blood flow.
All of the patients presented with chestpain , and they are all in triage. Remember, in diffuse subendocardial ischemia with widespread ST-depression there may b e ST-E in lead s aVR and V1. There are well formed R-waves with good voltage/amplitude which is uncommon for ischemia. True Positive ECG#2 : Also sinus rhythm.
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7].
When I was shown this ECG, I said it looks like such widespread ischemia that is might be a left main occlusion, or LM ischemia plus circumflex occlusion (high lateral and posterior OMI). Here are some cases of RBBB with LAFB: What is the Diagnosis in this 70-something with ChestPain? There is STE in aVR.
This includes sinus arrhythmia — in which there is often slight variation in the P-P interval. This slight variation in sinus P wave regularity tends to be greater when a 2nd- or 3rd-degree AV block is present ( called ventriculophasic sinus arrhythmia — as shown in ECG Blog #344 ). For clarity — I have done this in Figure-4.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. The ECG cannot diagnose the etiology of ischemia; it only the presence of ischemia, from whatever etiology.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. Patient 2 was seen immediately after patient 1 by the same cardiologist.
This is the prehospital ECG from an 81 year old man with acute chestpain. Arrhythmia? Today’s case recalled that scenario for me, in that it features recognition of an arrhythmia that fooled ED staff into thinking the ECG was showing an acute infarction. The medics did NOT activate the cath lab. Would you give lytics?
Chest trauma was suspected on initial exam. The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma? ST depression. Myocardial Contusion?
The presenting complaint was chestpain — and the patient collapsed soon after arrival in the ED. Shark Fin" ST segment elevation is most often a sign of severe transmural ischemia that results from acute coronary occlusion. QUESTION: A cardiologist interpreted the rhythm in Figure-1 as VT ( V entricular T achycardia ).
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy?
This middle aged male with h/o GERD but also h/o stents presented to the ED with chestpain. The initial troponin I returned at 1500 ng/L and another ECG was recorded as the patient complained of 9/10 chestpain at 10 hours after the first Now the T-wave in III is fully upright, suggesting re-occlusion.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. Anything more on history?
There was no chestpain. Extensive conduction system abnormalities can have various causes (ischemia, genetic, infectious, amyloid, etc). VT is the second most common presenting arrhythmia. Vaso or inotropic medications are not harmless, and can precipitate life threatening arrhythmias.
If you experience any symptoms, such as chestpain, dizziness, unusual tiredness or fatigue, shortness of breath, or irregular heartbeat, your doctor would want you to go for an ECG test to find out the underlying cause. Arrhythmia In simple words, arrhythmia refers to an irregular heartbeat.
No chestpain. Figure-1: The initial ECG in today's case — obtained from an 86-year old man with presyncope, but no chestpain. ( The other main consideration — is to take another look at the 12-lead ECG, and assess this for recent ischemia or infarction. Figure-5: Laddergram illustration of today's arrhythmia. =
RVOT VT: A 40-something without past history presents with wide complex tachycardia and crushing chestpain Regular Wide Complex Tachycardia. He got an MR, however that showed no scar or evidence of AVRD and he had a stress test with no evidence of inducible ischemia with almost 20 METs." There is no inferior axis.
If it is a chestpain patient, I would get a formal echo and serial ECGs. There were no others: Notice the similarities to the ECG above, confirming that they are baseline Then he sent the clinical history, which was of a malfunctioning ICD, but without any chestpain or SOB. And look for an old EKG."
A 40-something woman had sudden chestpain. Figure-1: Initial ECG, obtained pre-hospital from this 40-ish year old woman with new-onset chestpain ( See text ). The presence of such J waves may be associated with malignant ventricular arrhythmias. She called 911. But which myocardial walls are affected?
She did notice something slightly wrong subjectively, but had no palpitations, chestpain, or SOB, or any other symptom. The Role of Sinus Arrhythmia: I found it interesting to compare the long lead II rhythm strips in the 3 serial tracings from today’s case ( Figure-1 ). She was on no medications. Potassium was normal.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content