This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chestpain. He was eating lunch when he had sudden onset chest pressure, 9/10, radiating to his back, with sweating and numbness in both hands.
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. Inclusion criteria were chestpain, at least 2 serial cTnI in 24 hours, sinus rhythm , and at least 1 ECG.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
The word arrhythmia comes from two Greek words. So arrhythmia literally means absence or loss of rhythm. A cardiac arrhythmia therefore means loss of cardiac rhythm. These include breathlessness, chestpain, dizziness or even blackouts. Most dysrhythmias once identified are easily treatable.
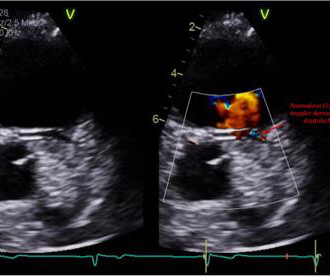
Electrocardiogram in clinic showed sinus arrhythmia with early repolarization and no ischemic changes. The echocardiogram showed normal cardiac structure and function, however, there was a concern for possible anomalous origin of the left coronary artery. Invasive coronary angiography ruled out luminal narrowing or dynamic compression.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. Patient 2 was seen immediately after patient 1 by the same cardiologist.
Hopefully a repeat echocardiogram will be performed outpatient. ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. 1900: RBBB and LAFB are almost fully resolved.
Later, I found old ECGs: 5 month prior in clinic: V5 and V6 look like OMI 9 months prior in clinic with no chest symptoms: V5 and V6 look like OMI 1 year prior in the ED with chestpain: V5 and V6 sure look like a STEMI For this ECG and chestpain in the ED, the Cath lab activated. But the angiogram was clean.
Yes, COVID-19 symptoms can resemble a heart attack, including chestpain, shortness of breath, and changes in echocardiogram or EKG. Myocarditis symptoms can also mimic a heart attack, and small blood clots may cause pain. Can COVID-19 symptoms mimic a heart attack?
On the other hand — the ST elevation seen in lead V1 is perfectly consistent with LVH and LV "strain" ( ie, The shape of this ST-T wave in lead V1, in association with the deep S wave in this lead — is a mirror-image opposite picture of the typical expected appearance of LVH with "strain" in a lateral chest lead ).
No patient with chestpain should be sent home without troponin testing. An echocardiogram showed severely reduced global systolic function with an EF of 20-25% and an LV apical thrombus. An echocardiogram showed an EF of 20-25%. Three months later, he had a follow up appointment for a reassessment of his LV function.
This middle aged male with h/o GERD but also h/o stents presented to the ED with chestpain. The initial troponin I returned at 1500 ng/L and another ECG was recorded as the patient complained of 9/10 chestpain at 10 hours after the first Now the T-wave in III is fully upright, suggesting re-occlusion.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
The pneumothorax was expanded with a chest tube At 17 hours, another ECG was recorded: It is now much less dramatic and has the morphology of Type 2 Brugada The hs troponin I peaked at 6500 ng/L -- this strongly suggests myocardial contusion. An echocardiogram was done. He has a family history concerning for arrhythmia.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. See this case: what do you think the echocardiogram shows in this case?
She reports that she is now unable to vagal out of her palpitations and is having shortness of breath and dull chestpain. She had an echocardiogram which was normal. Patients should be offered a choice for a trial of medication vs ablation for this non-life-threatening arrhythmia. Her initial EKG is below.
Echocardiogram: Estimated left ventricular ejection fraction, lower limits of normal; 45-50%. There are 6 KEY parameters to consider in systematic assessment of any arrhythmia. Tele Monitor: Normal sinus rhythm throughout, no ectopic atrial or ventricular beats. Regional wall motion abnormality-inferior/inferoseptum: akinetic.
Echocardiogram showed LVEF 66% with normal wall motion and normal diastolic function. He did not remember whether he had experienced any chestpain. Two subsequent troponins were down trending. Within a few days, the patient was extubated and was neurologically intact.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. Altogether, this strongly suggests inferolateral OMI, particularly in a patient with acute chestpain.
Arrhythmias (Irregular Heartbeats) Persistent abnormal heart rhythms can disrupt the heart’s pumping efficiency, eventually causing it to enlarge to maintain blood flow. Chest X-Ray A chest X-ray is often the first imaging test conducted, as it can reveal whether the heart is enlarged and by how much.
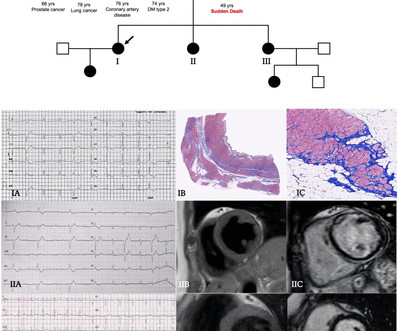
Twenty-one (41%) had normal echocardiogram, 13 (25%) a hypokinetic non-dilated cardiomyopathy (HNDC) and 17 (33%) a dilated cardiomyopathy (DCM). Clinical contexts leading to diagnosis were SCD in 3 (6%), ventricular arrhythmias in 15 (29%), chestpain in 8 (15%), heart failure in 6 (12%) and familial screening in 20 (38%).
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Formal echocardiogram showed normal EF, no wall motion abnormalities, no pericardial effusion. There was a 0.9%
However, an echocardiogram is a different test, also conducted for heart activity. If you experience any symptoms, such as chestpain, dizziness, unusual tiredness or fatigue, shortness of breath, or irregular heartbeat, your doctor would want you to go for an ECG test to find out the underlying cause.
He has never had any chestpain. Echocardiogram is indicated (Correct) C. Start aspirin and Plavix Correct answer: (B) (B) Echocardiogram is indicated. He has no known prior medical history and does not take any medications. He complains of occasional shortness of breath on walking more than 2 blocks.
A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. It was from a patient with chestpain: Note the obvious Brugada pattern. Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias.
This middle-aged man with no cardiac history but with significant history of methamphetamin and alcohol use presented with chestpain and SOB, worsening over days, with orthopnea. Later, he underwent a formal echocardiogram: Very severe left ventricular enlargement (LVED diameter 7.4 BP:143/99, Pulse 109, Temp 37.2 °C
He was concerned because he had chestpain after his first mRNA vaccine and was uncomfortable with the risks of a second mRNA dose. He subsequently describes having sharp chestpain over the next few weeks. The pain resolved a few weeks later. He emphatically denies any history of cardiopulmonary disease.
Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). The most recent and probably best study is this: Canadian Syncope Arrhythmia Risk Score.
Written by Willy Frick A man in his 60s with hypertension and prior stroke presented with three days of crushing chestpain. He reported intermittent chestpain for the last few months, but never lasting this long. The cardiology consultant notes that pain is "almost resolved." There is active infarction.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content