This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Coronary artery spasm (CAS), or Prinzmetal angina, is a recognised cause of myocardial ischaemia in non-obstructed coronary arteries which typically presents with anginal chestpain. The patient presented with recurrent palpitations and pre-syncope, with no chestpain.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. There are three mechanisms of arrhythmia: automatic, re-entry, and triggered.
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chestpain. He was eating lunch when he had sudden onset chest pressure, 9/10, radiating to his back, with sweating and numbness in both hands.
No ChestPain, but somnolent. The fact that this is syncope makes give it a far lower pretest probability than chestpain, but it was really more than syncope, as the patient actually underwent CPR and had hypotension on arrival of EMS. Here is the ED ECG (a photo of the paper printout) What do you think?
Written by Willy Frick A man in his 50s with history of hypertension, hyperlipidemia, and a 30 pack-year smoking history presented to the ER with 1 hour of acute onset, severe chestpain and diaphoresis. His ECG is shown: What do you think? What do you think? Given the R-R interval = 1160 msecs.
Click here to sign up for Queen of Hearts Access Case A 58-year-old woman presented to the ED with burning chestpain that started 2-3 hours earlier while sitting on a porch swing. In any case, it is diagnostic of OMI in a chestpain patient.
He did not remember whether he had experienced any chestpain. This is a critically important determination because of the 2017 AHA/ACC/HRS Guidelines for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death. Within a few days, the patient was extubated and was neurologically intact.
Signs include: Sudden loss of consciousness No pulse or breathing Collapse without prior chestpain or discomfort If someone experiences sudden cardiac arrest, it is crucial to begin CPR immediately and call the local emergency number. Without prompt treatment, parts of the heart muscle may become damaged or die.
The primary endpoint was the incidence of device syndrome, a composite of patient-reported symptoms (chestpain, palpitations, migraines, dyspnea, and rash).Results:Of No significant differences were observed in documented arrhythmias, bleeding, or stroke. Nickel hypersensitivity was assessed using skin patch testing.
I went to the patient's chart: Elderly woman with stuttering chestpain and SOB, and dizziness. Tall R wave in lead V1 and/or early transition in the chest leads ( reflecting increased "septal" forces ). WPW Cardiac arrhythmias ( including AFib ). What do you think now? Abnormal ST-T wave abnormalities.
Whenever a patient does not have chestpain, the pre-test probability of OMI is diminished. Of course SOB, jaw pain, shoulder pain, etc can be a result of OMI, but the pretest probability is less and so you must scrutinize further. Lethal arrhythmias may be a terminal event ( VT/VFib; Asystole ).
years and experiencing chestpain. Most cases were male and involved chestpain. Myocarditis, an inflammation in the myocardium, can cause dilated cardiomyopathy, acute arrhythmia, and heart failure. The prognosis was generally good, with no reported death.
The individual relationship between fatal arrhythmias and cardiac function abnormalities in predicting cardiac death risk has rarely been explored. Methods We retrospectively analyzed the measurements at rest for 191 patients with acute chestpain (ACP) magnetocardiographically.
Case sent by Logan Stark MD, written by Pendell Meyers A woman in her 70s presented with acute chestpain. Or perhaps the group beating is simply the result of sinus arrhythmia that by chance results in alternating R-R intervals of very similar size? No prior ECG was available. Here is her triage ECG: What do you think?
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. Inclusion criteria were chestpain, at least 2 serial cTnI in 24 hours, sinus rhythm , and at least 1 ECG.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. Altogether, this strongly suggests inferolateral OMI, particularly in a patient with acute chestpain.
A previously healthy middle-aged male presented shortly after the acute onset of chestpain very shortly before calling 911. On arrival, he was pain free: What do you think? Jerry Jones commented: "Any ST depression on the ECG of a patient with chestpain credible for ACS represents a reciprocal change until proved otherwise."
Written by Jesse McLaren A previously healthy 60 year old developed exertional chestpain with diaphoresis, and called EMS. There’s sinus arrhythmia with normal conduction, normal axis and normal voltages. Here’s the EMS ECG, digitized with PM cardio. What do you think? There’s loss of R waves in V2-3 with hyperacute waves V1-5.
Shortly after receiving epinephrine, the patient developed new leg cramps and chestpain. The chestpain was described as sharp and radiated to both arms. During active chestpain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF.
A 50-something presented with acute chestpain. MY Thoughts on today’s “quick-look ECG” are the following: There is sinus arrhythmia. Here is her ED ECG. It was texted to me while I was out and about. He wrote: "Steve, what do you think about hyperacute T waves in this? 54-year-old female with CP. What do you think, Dear Reader?
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. He has a medical hx notable for hypertension, hyperlipidemia and previous tobacco use disorder.
Currently, he has no complaints: no palpitations, no shortness of breath, no syncope, no chestpain. There is a non-respiratory sinus arrhythmia present, which is essentially the minimal variant of a sick sinus syndrome. This is the ECG of an 81-year-old man with hypertension.
The computer called it a normal ECG Algorithm unknown Aside : [There is some "sinus arrhythmia", which is indeed a normal finding. Sinus arrhythmia is sinus rhythm whose rate varies with respiration. If the longest P-P interval is 120 ms greater than the shortest, it is sinus arrhythmia. Burning pain subxiphoid and into throat."
The patient presented with chestpain. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. Only 5-18% of ED patients with chestpain have a myocardial infarction of any kind. Is it Brugada pattern?
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
Written by Jesse McLaren, with edits from Smith and Grauer A 60 year old with no past medical history presented with two hours of chestpain radiating to the left arm, with normal vitals. Unfortunately, the reality is — that many ( most ) WPW patients who present with chestpain do not manifest intermittent preexcitation.
There is a patient with persistent chestpain and an initial troponin I over 52 ng/L; 52 ng/L has an approximate 70% PPV for acute type I MI in a chestpain patient. Pain was severe and persistent. CT angiography chest assessing for PE and dissection negative. Heparin drip was initiated. Is there STEMI?
It is from a 50-something with chestpain: What do you think? In my opinion — AI is not yet "there" with regard to interpretation of complex cardiac arrhythmias. I like to start my ECG assessment in patients with new chestpain by looking for at least 1 or 2 leads that I know are definitely abnormal.
The patient has acute chestpain. Instead — my thoughts were as follows: The rhythm is sinus , with marked bradycardia and a component of sinus arrhythmia. Tall R wave in lead V1 and/or early transition in the chest leads ( reflecting increased "septal" forces ). WPW Cardiac arrhythmias ( especially AFib ).
The word arrhythmia comes from two Greek words. So arrhythmia literally means absence or loss of rhythm. A cardiac arrhythmia therefore means loss of cardiac rhythm. These include breathlessness, chestpain, dizziness or even blackouts. appeared first on Dr Sanjay Gupta Cardiologist.
Written by Pendell Meyers A woman in her 50s presented with acute chestpain and lightheadedness since the past several hours. For our readers who enjoy the challenge of interpreting cardiac arrhythmias — today’s case offers a “gold mine” of PEARLS regarding the recognition of AV Wenckebach.
In the evening, a middle-aged man complained of chestpain at the nursing home. His chestpain was vague. He mentioned "cancer" and "chest". I’ll focus my comments on arrhythmia diagnosis. P EARL # 2 : In my experience — the most commonly overlooked arrhythmia ( by far! ) Fluids were started.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. However, he suddenly developed a series of malignant ventricular arrhythmias.
She was hemodynamically stable — and did not have chestpain, lightheadedness or syncope. With P waves labeled — Isn't it now much easier to appreciate that the atrial rhythm is quite regular ( with no more than a slight sinus arrhythmia )? For those with a special interest in cardiac arrhythmias — READ ON! —
My THOUGHTS on ECG #1: We are told that the patient in today’s case had an episode of severe chestpain 3 nights prior to admission. This should include details regarding the dosing regimen — the nature of the ventricular arrhythmia being treated — and the patient’s “baseline” QTc at steady state for his/her current Sotalol dose.
Currently, he has no complaints: no palpitations, no shortness of breath, no syncope, no chestpain. There is a non-respiratory sinus arrhythmia present, which is essentially the minimal variant of a sick sinus syndrome. This is the ECG of an 81-year-old man with hypertension.
This was written by Magnus Nossen, from Norway, with comments and additions by Smith A 50 something smoker with no previous medical hx contacted EMS due to acute onset chestpain. Upon EMS arrival the patient appeared acutely ill and complained of chestpain. Of academic interest — are the arrhythmias that developed.
Note the Timed Contents that I detail below facilitate finding specific material. == ECG Podcast #4 — All About Comparison ECGs for 12-Leads and Arrhythmias ( Comparing ECGs seems so "easy" to do — but so often is not done correctly! ) — published by Mayo Clinic CV Podcast Series on 5/21/2024 ( 35 minutes ). What are the problems?
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7].
BackgroundAmiodarone is a class III antiarrhythmic drug that is commonly used in the clinic to treat ventricular arrhythmias and atrial fibrillation. Despite normal annual check-ups, she developed abnormal liver and thyroid function tests, and imaging revealed lung and liver changes suggestive of amiodarone toxicity.
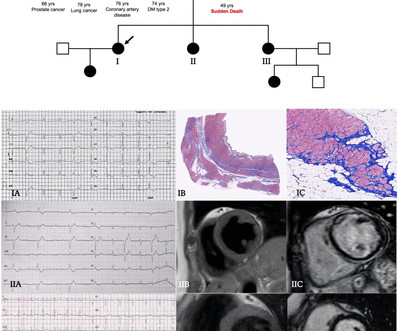
Clinical contexts leading to diagnosis were SCD in 3 (6%), ventricular arrhythmias in 15 (29%), chestpain in 8 (15%), heart failure in 6 (12%) and familial screening in 20 (38%). Of 47 tested patients, 29 (62%) were carriers of a pathogenic/likely pathogenic DNA variant.
And regarding arrhythmias: For more on the regular WCT — See My Comment in the May 5, 2020 post and in the April 15, 2020 post in Dr. Smith's ECG Blog. 11:35 — My views on: Will the computer ever be able to interpret complex arrhythmias? 14:45 — Using my definition — Are YOU an “ expert ” ECG interpreter? What are the problems?
Patients may feel a fluttering in the chest, chestpain, shortness of breath and dizziness or lightheadedness as a result. It represents a unique opportunity to advance our therapy to the next level and potentially be able to treat patients with ventricular arrhythmias in a better way, without destroying healthy heart tissue.
We have long known that pulsed field ablation could open up an entirely new frontier in how we treat people battling the most complex cardiac arrhythmias. In addition to upcoming procedures in markets across Asia Pacific and Europe, Abbott anticipates approval for its U.S. chief medical officer of Abbott's electrophysiology business.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content