This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Cingolani, director of Cardiogenetics and Preclinical Research in the Department of Cardiology in the Smidt Heart Institute at Cedars-Sinai, is exploring new ways to help patients with ventricular tachycardia (VT), a recurring, abnormally fast and irregular heartbeat that starts in the lower chambers, or ventricles, of the heart.
But cardiacarrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. After cardiacarrest, I ALWAYS wait 15 minutes after an ECG like this and record another. See these related cases: Cardiacarrest, defibrillated, diffuse ST depression and ST Elevation in aVR.
While on telemetry monitoring he suffered cardiacarrest and was resuscitated. What ECG finding may have contributed to (or precipitated) the cardiacarrest? Learning points : Takotsubo can lead to cardiacarrest from ventricular arrhythmia. There are no clear signs of OMI. There is a prolonged QTc.
He developed cardiacarrest shortly after the ECG in Figure-1 was recorded. What is the most likely cause of this arrhythmia? IMPRESSION: Given the presence of a wide tachycardia — with 2 distinct QRS morphologies, and no sign of P waves — a presumed diagnosis of B i D irectional Ventricular Tachycardia has to be made.
See this post: How a pause can cause cardiacarrest 2. In this specific case, Left Bundle Branch (LBB) area pacing was pursued to achieve cardiac resynchronization. (J Even with tachycardia and a paced QRS duration of ~0.16 The plan: 1. Place temporary pacemaker 3. Discontinue amiodarone, since it prolongs the QT 4.
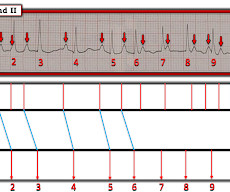
A series of cardiacarrhythmias were seen during the course of her resuscitation — including the interesting arrhythmia shown in the long lead II of Figure-1. What is the cardiac rhythm shown in the long lead II rhythm strip? PEARL # 5: The simple act of labeling P waves can be invaluable for solving an arrhythmia.
A 60-something woman presented after a witnessed cardiacarrest. This is commonly found after epinephrine for cardiacarrest, but could have been pre-existing and a possible contributing factor to cardiacarrest. Final Diagnosis: CardiacArrest due to Torsades from long QT of unknown etiology.
However, he suddenly developed a series of malignant ventricular arrhythmias. This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). Below are printouts of some of the arrhythmias recorded. What do you think?
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. T wave alternans is a harbinger of cardiac instability and TdP. (3) No ischemic ST changes.
PEARL # 2: It is important to be aware that " not every arrhythmia obeys the rules!" As a result — We sometimes need to think "out of the box" in order to come up with the most plausible explanation for a given arrhythmia. PEARL # 3: Although ATach is usually a fairly regular atrial rhythm — there may at times be some irregularity.
ECG is consistent with severe hypokalemia and/or hypomagnesemia causing prolonged QT (QU) at high risk of Torsades (which is polymorphic ventricular tachycardia in the setting of a long QT interval). Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management CardiacArrest.
A few decades ago all sudden cardiacarrests with documented ventricular fibrillation (VF) and structurally normal hearts were diagnosed as idiopathic ventricular fibrillation (IVF).
Blood was drawn , and the patient was promptly placed in a room to be seen — but on entering, the ED physician found her unresponsive in cardiacarrest. Do you see any indication on this ECG of WHY this patient was about to arrest? Is there any indication on this ECG of WHY this patient shortly after had a cardiacarrest?
Since the patient was stable and tolerating the arrhythmia it was decided to treat with IV Amiodarone for medical conversion. The 2019 ESC Guidelines for the management of patients with supraventricular tachycardia indicated that IV Amiodarone should not be considered in these populations. Smith : What do you think? What is it?
See here for management of Polymorphic Ventricular Tachycardia , which includes Torsades. IV administration of potassium is indicated when arrhythmias are present or hypokalemia is severe (potassium level of less than 2.5 If cardiacarrest from hypokalemia is imminent (i.e., Could the dysrhythmias have been prevented?
The arrhythmia spontaneously converted before defibrillation was achieved. This patient is actively dying from a left main coronary artery OMI and cardiacarrest from VT/VF or PEA is imminent! Complete LMCA occlusion is associated with clinical shock and/or cardiacarrest.
Here is the ECG: Sinus tachycardia. IV administration of potassium is indicated when arrhythmias are present or hypokalemia is severe (potassium level of less than 2.5 If cardiacarrest from hypokalemia is imminent (i.e., malignant ventricular arrhythmias are present), rapid replacement of potassium is required.
Arrhythmia In simple words, arrhythmia refers to an irregular heartbeat. A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. CardiacarrestCardiacarrest is a medical emergency in which the heart stops pumping blood to the body.
Similarly, you may use our , app to adjust the paper speed along with amplification to read the slightest changes, especially for conditions like tachycardia and bradycardia. AI recognizing cardiacarrests in emergency calls. Recently, hospitals have failed to identify 25% of cases of cardiacarrest.
Is it ventricular tachycardia (VT) due to hyperK or is it a supraventricular rhythm with hyperK? Here are other posts on hyperK, large calcium doses for hyperK, and ventricular tachycardia in hyperK Weakness, prolonged PR interval, wide complex, ventricular tachycardia Very Wide and Very Fast, What is it? How would you treat?
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below. Arch Intern Med.
Smith: This bizarre ECG looks like a post cardiacarrest ECG with probable acidosis or hyperkalemia in addition to OMI. The patient died of cardiogenic shock within 24 hours despite mechanical circulatory support. Below the J-point is marked out showing the ST pathologic deviations. What was the pH and K?
NOTE: As discussed in detail in ECG Blog #108 — " A IVR" is an "enhanced" ventricular ectopic rhythm that occurs faster than the intrinsic ventricular escape rate ( which is typically between 20-40/minute ) — but slower than hemodynamically significant Ventricular Tachycardia ( ie, VT at rates >130-140/minute ).
This is the proposed mechanism of precipitation of arrhythmias in Brugada syndrome during febrile episodes. There is a potential risk for drug challenge in that life threatening ventricular arrhythmias could be precipitated. This leads to shortening of action potential duration. With proper precautions, risk can be reduced.
He has a family history concerning for arrhythmia. Given the circumstances of his car crash, we presume it was due to an underlying arrhythmia. He has a family history concerning for arrhythmia with his father requiring some sort of device (PPM, ICD, unclear) at a young age.
Thirty-six patients (36%) presented with cardiacarrest, and 78% (28/36) underwent emergent angiography. Systematic Assessment of the ECG in Figure-1: My Descriptive Analysis of ECG findings in Figure-1 is as follows: Sinus tachycardia at ~110/minute. Results Emergent angiography was performed in 80% (79/99) of patients.
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7]. There was a 0.9% Circulation, 117, 1890–1893. [3]:
The ECG shows sinus tachycardia, a narrow, low voltage QRS with alternating amplitudes, no peaked T waves, no QT prolongation, and some minimal ST elevation in II, III, and aVF (without significant reciprocal STD or T wave inversion in aVL). It is difficult to tell if there is collapse during diastole due to the patient’s tachycardia.
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. Her temperature was 106 degrees. As part of the workup, she underwent an ECG.
While traditionally described as “benign early repolarization”, they have been associated with J wave syndromes along with Brugada syndrome, causing ventricular arrhythmias (1, 2). The relationship between J wave and ventricular tachycardia during Takotsubo cardiomyopathy. Indian Pacing Electrophysiol J 2004 Antzelevitch C, Yan G.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content