This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 60-something woman presented after a witnessed cardiacarrest. This is commonly found after epinephrine for cardiacarrest, but could have been pre-existing and a possible contributing factor to cardiacarrest. Final Diagnosis: CardiacArrest due to Torsades from long QT of unknown etiology.
See this post: How a pause can cause cardiacarrest 2. Place temporary pacemaker 3. In this specific case, Left Bundle Branch (LBB) area pacing was pursued to achieve cardiac resynchronization. The plan: 1. Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses.
Click here to sign up for Queen of Hearts Access Here is the cardiologist's formal interpretation : "sinus rhythm with marked sinus arrhythmia, left ventricular hypertrophy with repolarization abnormality, and anteroseptal infarct, age undetermined." About 45 minutes after the second EKG, the patient was found in cardiacarrest.
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. T-wave alternans and the susceptibility to ventricular arrhythmias. Teaching Points: 1. 2017.3191.
Blood was drawn , and the patient was promptly placed in a room to be seen — but on entering, the ED physician found her unresponsive in cardiacarrest. Do you see any indication on this ECG of WHY this patient was about to arrest? Is there any indication on this ECG of WHY this patient shortly after had a cardiacarrest?
My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. Given this patient's older age — if nothing "fixable" is found, she most likely has SSS ( S ick S inus S yndrome ) and will need a pacemaker ( See ECG Blog #342 for more on SSS ).
My thoughts were the following: ECGs #1 and #2 showed a completely unreliable sinus pacemaker, with presumed high-grade 2nd-degree AV block — and frequent resultant pauses of over 2 seconds ( that would have been even longer had it not been for intermittent relief from the atrial escape focus ). What Does this All Mean?
However, he suddenly developed a series of malignant ventricular arrhythmias. Below are printouts of some of the arrhythmias recorded. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. The arrhythmia starts with a PVC having a short coupling interval.
Arrhythmia In simple words, arrhythmia refers to an irregular heartbeat. CardiacarrestCardiacarrest is a medical emergency in which the heart stops pumping blood to the body. Electrocardiogram, echocardiogram, and some other tests are done for patients with cardiacarrest.
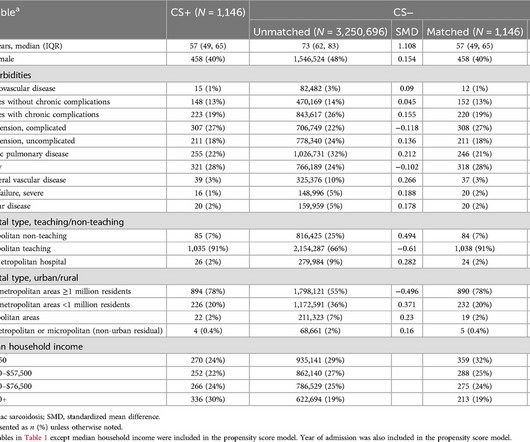
Hospitalizations with a primary diagnosis suggestive of CS (HF/cardiomyopathy, cardiacarrest, arrhythmias, or heart block) were categorized into cases with and without CS as a secondary diagnosis (CS+ and CS−, respectively). The CS+ cohort included patients who were younger and more often male.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content