This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Notwithstanding many insightful observations, the electrocardiogram (ECG) arguably ignited the big bang in our understanding of cardiac arrhythmias. Using ECG recording and deductive reasoning, our teachers and predecessors classified the bradycardias and tachycardias and proposed many mechanisms, subsequently proven to be correct.
Sinus tachycardia – sinus rhythm above 100 bpm is a sinus tachycardia. Sinus bradycardia – sinus rhythm below 60 bpm is a sinus bradycardia. Ventricular tachycardia – more than 7 consecutive complexes originating from ventricles at a rate of > 100 bpm. Usually does not exceed 160 bpm.
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. As described above by Dr. Smith Pacing in today's case is an effective intervention as doing so prevents the bradycardia and pauses that are likely to precipitate additional episodes of Torsades de Pointes. (
Ventricular tachycardia is a potentially life threatening cardiac arrhythmia. On the ECG, ventricular tachycardia can be defined as three or more ventricular ectopic beats occurring in a sequence at a rate more than 100 per minute. Another rare form of ventricular tachycardia is bidirectional ventricular tachycardia.
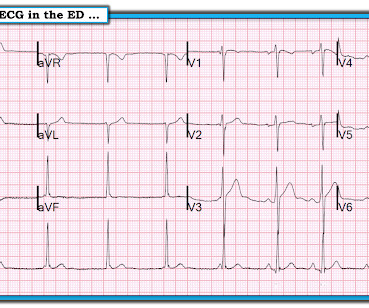
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. The Initial ECG in Today's Case: As per Dr. Meyers — the initial ECG in today's case shows sinus tachycardia with bifascicular block ( = RBBB/LAHB ). Sinus Tachycardia ( common in any trauma patient. ). QTc prolongation.
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. It is hard to make out P waves but you can see them best in V2, and notches in the T waves in other leads - this is a sinus tachycardia with a very long PR interval indicating first degree block.
Learning objectives To review the potential arrhythmia complications during pregnancy and puerperium in women with and without known cardiovascular disease. To recognise arrhythmia conditions associated with a high risk of pregnancy-related cardiac complications for which intervention before considering pregnancy is appropriate.
KEY Point: Knowing that the most commonly overlooked arrhythmia is AFlutter — suggests that the BEST way to avoid missing the diagnosis of AFlutter is simply to THINK of AFlutter whenever you have a regular SVT at a rate close to 150/minute ( in which you do not clearly see upright sinus P waves in lead II ). And a Final Tracing.
to 1828 msec. ) — which corresponds to a variation in the rate of sinus bradycardia from 36-to-33/minute. This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute.
Wide-complex tachycardia: VT or aberrant, or "other?" A wide-complex tachycardia in an older patient must immediately suggest ventricular tachycardia. Sinus tachycardia with aberrancy was unlikely as the rate was consistently 150 bpm, without spontaneous variation. second ), in which the tachycardia is sustained.
Initial ECG in the ED: Presenting ECG : Wide-complex tachycardia at a rate about 200. This is overwhelmingly likely to be ventricular tachycardia, even if only age and medical history are considered. Nevertheless, the widths of both the QRS complex and the RS duration are similar in both the old ECG and the tachycardia.
Early detection of conditions like AFib, bradycardia, or tachycardia allows patients to address issues before they become critical. Risk Reduction Data from wearables can identify potential risks, such as undiagnosed arrhythmias or hypertension, allowing healthcare teams to address these issues before surgery.
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. Analysis: there is a wide complex tachycardia. This was the interpretation I put into the system: WIDE COMPLEX TACHYCARDIA. It is regular.
during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. The easy way to remember the arrhythmias most commonly associated with SSS is to think of what one might expect if the SA node became sick. The indication for pacemaker placement with SSS is symptomatic bradycardia.
== P EARL # 1: The easiest way to instantly enhance your arrhythmia interpretation skills is by using calipers. The cardiologist who does not regularly use calipers for interpretation of complex arrhythmias is a cardiologist who will miss the diagnosis on more than a few occasions. Using calipers will NOT slow you down.
Most of the time with AV block — the atrial rhythm will be regular ( or at least almost regular — if there is an underlying sinus arrhythmia ). PEARL # 5: As noted above — today's arrhythmia appears to represent some form of 2nd-degree AV block. Figure-4: I needed to draw a laddergram. .
Similarly, you may use our , app to adjust the paper speed along with amplification to read the slightest changes, especially for conditions like tachycardia and bradycardia. Alternatively, it also helps enhance arrhythmia management with coronary artery disease. It improves the prediction model for myocardial scar mass.
Learning points : Takotsubo can lead to cardiac arrest from ventricular arrhythmia. But there are 3 other wide beats in the tachycardia that begins with beat #6 ( = beats #7; 13,14 ). The QTc then gradually shortened over the course of several days as is usual for stress cardiomyopathy.
He has a family history concerning for arrhythmia. Given the circumstances of his car crash, we presume it was due to an underlying arrhythmia. He has a family history concerning for arrhythmia with his father requiring some sort of device (PPM, ICD, unclear) at a young age.
Additionally, his cardiac telemetry monitor showed runs of accelerated idioventricular rhythm, a benign arrhythmia often associated with coronary reperfusion. He had multiple episodes of bradycardia and nonsustained ventricular tachycardia. As expected, the patient reported total resolution of pain by the time he got to the ED.
Therefore, she underwent temporary pacemaker placement and overdrive pacing at a rate of 90 bpm to keep the heart rate up in order to prevent these PVCs triggering ventricular arrhythmia. Hypokalemia was unlikely because she continued to have ventricular arrhythmia despite of correcting electrolytes.
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. VT is the second most common presenting arrhythmia. Vaso or inotropic medications are not harmless, and can precipitate life threatening arrhythmias. She was started on isoprenalin (isoproterenol).
However, he suddenly developed a series of malignant ventricular arrhythmias. This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). Below are printouts of some of the arrhythmias recorded. What do you think?
There are three mechanisms of arrhythmia: automatic, re-entry, and triggered. The most common triggered arrhythmia is Torsades de Pointes. Automatic activity refers to enhanced pacemaking function (typically from a non sinus node source), for example atrial tachycardia. This has been discussed many times before on this blog.
Introduction The incidence of arrhythmia in heart failure with non-reduced ejection fraction (HFnon-rEF) in patients who have a history of hospitalisation is unclear. Methods and analysis This is a multicentre single arm study to evaluate the usefulness of ILR for detecting arrhythmia.
There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Torsades in acquired long QT is much more likely in bradycardia because the QT interval following a long pause is longer still. See here for management of Polymorphic Ventricular Tachycardia , which includes Torsades.
ECG is consistent with severe hypokalemia and/or hypomagnesemia causing prolonged QT (QU) at high risk of Torsades (which is polymorphic ventricular tachycardia in the setting of a long QT interval). Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management Cardiac Arrest. Is it STEMI?
The arrhythmia spontaneously converted before defibrillation was achieved. As per Dr. Nossen — today's initial ECG ( LEFT tracing in Figure-2 ) shows sinus bradycardia with QRS widening due to bifascicular block ( RBBB/LAHB ). The patient was rushed to the nearest emergency department (non-PCI facility) for stabilization.
I completely agree with Dr. Nossen that in this patient with new CP and sinus tachycardia with LAHB — that the T waves in each of the inferior leads are hyperacute ( ie, clearly disproportionately "bulky" given size of the QRS in these leads ). — and which other patient(s) need to be seen as soon as possible to figure out what is going on?
Arrhythmia In simple words, arrhythmia refers to an irregular heartbeat. A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. If your heart beats too slowly, too quickly, or irregularly, an ECG will easily detect it.
It can automatically detect life threatening ventricular arrhythmias and treat them, either with a shock or, sometimes by overdrive pacing. And, after the shock, if there is bradycardia, it can be covered by these two pacing electrodes, one at the tip, and one proximal to it. These are high voltage, defibrillator shock coils.
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7]. There was a 0.9% Circulation, 117, 1890–1893. [3]:
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful.
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. Her temperature was 106 degrees. As part of the workup, she underwent an ECG.
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). The possibility of an ischemic cause of the ventricular arrhythmia has to be considered! A workup was undertaken in search of a cause of the patient's ventricular arrhythmia. No PVCs are seen.
This ECG shows a sinus bradycardia with a normal conduction pattern (normal PR, normal QRS, and normal QTc), normal axis, normal R-wave progression, normal voltages. Hypothermia can also produce bradycardia and J waves, with a pseudo-STEMI pattern. ECG met STEMI criteria and was labeled STEMI by computer interpretation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content