This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
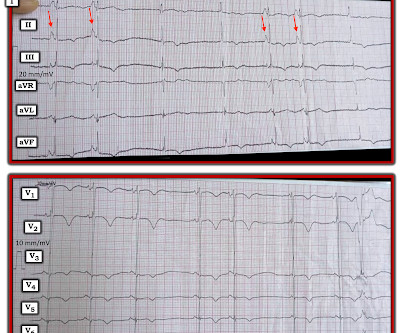
For full discussion of the case — CLICK HERE — ECG Rhythm Overview: A 12-year-old boy was admitted to our hospital with severe myocardial dysfunction and chaotic rhythm with tachy- and bradycardic arrhythmias. Perhaps the patient has pulmonary hypertension and/or tricuspid regurgitation?
CT of the chest showed no pulmonary embolism but bibasilar infiltrates. Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. She was intubated. Bedside cardiac ultrasound showed moderately decreased LV function. The plan: 1. Place temporary pacemaker 3.
Q waves in association with RBBB are usually not seen in anterior leads unless there is pulmonary hypertension or anterior infarction. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). RBBB in blunt chest trauma seems to be indicative of several RV injury.
This middle-aged patient presented with SOB, weakness, and mild pulmonary edema. There are 3 etiologies I always think of with bradycardia and AV block: 1. In my experience the aspect of interpretation that computer algorithms do most poorly in, is interpretation of complex arrhythmias. This shows atrial fibrillation.
Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Mean baseline [K] p was 2.9
PVCs N ot generally considered abnormal ECG findings: Isolated PAC, First Degree AV Block, Sinus bradycardia at a rate of 35-45, and Nonspecific ST-T abnormalities (even if different from a previous ECG). Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful.
For many us, frying or freezing the atrial or pulmonary venous tissue would come to our mind first , overlooking systemic factors. We don’t need to think deep, to realize, modalities which take on this arrhythmia head-on has a minuscule role at the population level.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content