This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BackgroundThere have been few instances of symptomatic bradycardia-arrhythmia in the context of area postrema syndrome (APS), and some of them have been implanted permanent pacemakers. Brady-arrhythmia was presented in all patients, and 9 patients were implanted temporary or permanent pacemakers.
Interpreting the waves and detecting abnormalities: Typically, the heart conducts electricity in a pathway starting in the sinoatrial node (SA), our heart’s “natural pacemaker”, located in the wall of the right atrium. Sinus bradycardia – sinus rhythm below 60 bpm is a sinus bradycardia.
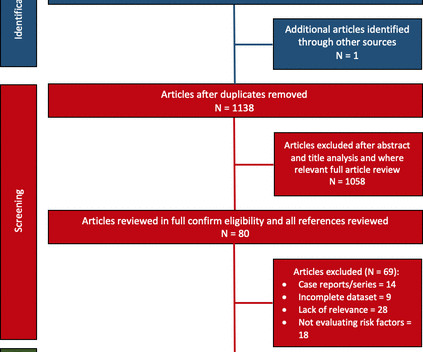
Cardiac accumulation triggers local tissue injury, electrical instability and arrhythmia. Objective We conducted a systematic review evaluating AF burden and bradycardia requiring permanent pacemaker (PPM) implantation and report any predictive risk factors identified. Study outcomes included AF or bradycardia requiring therapy.
For full discussion of the case — CLICK HERE — ECG Rhythm Overview: A 12-year-old boy was admitted to our hospital with severe myocardial dysfunction and chaotic rhythm with tachy- and bradycardic arrhythmias. In the meantime, a pacemaker may be needed. = There definitel are periods of bradycardia (so pacing may be needed for that).
Is a pacemaker needed? With P waves labeled — Isn't it now much easier to appreciate that the atrial rhythm is quite regular ( with no more than a slight sinus arrhythmia )? P utting I t A ll T ogether : The precise mechanism of today's arrhythmia is complex and difficult to determine. Is this " high -grade" AV block?
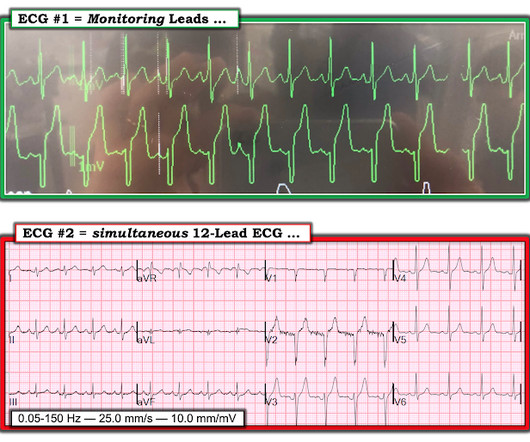
My thoughts were the following: ECGs #1 and #2 showed a completely unreliable sinus pacemaker, with presumed high-grade 2nd-degree AV block — and frequent resultant pauses of over 2 seconds ( that would have been even longer had it not been for intermittent relief from the atrial escape focus ). What Does this All Mean?
However, he suddenly developed a series of malignant ventricular arrhythmias. Below are printouts of some of the arrhythmias recorded. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. The arrhythmia starts with a PVC having a short coupling interval.
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. Place temporary pacemaker 3. There is ventricular bigeminy with bizarre appearing wide T-waves See even more striking cases of this at the bottom of the post. The plan: 1.
Written by Willy Frick A man in his 70s with a history of HFrEF and sick sinus syndrome s/p dual chamber pacemaker placement was admitted for overnight observation following outpatient placement of a mitral valve clip. This is unambiguous evidence of pacemaker malfunction. Imagine the pacemaker is set at a minimum rate of 60.
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. They knew she would need a pacemaker unless some transient and reversible cause was discovered. Once this happens, of course, the patient will require temporary or permanent pacemaker as soon as possible.
We admitted him for probable EP study and possible pacemaker. He underwent pacemaker placement and is doing fine. SSS is by far the most common reason for permanent pacemaker placement. during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. Learning Points: 1.
Introduction The incidence of arrhythmia in heart failure with non-reduced ejection fraction (HFnon-rEF) in patients who have a history of hospitalisation is unclear. Methods and analysis This is a multicentre single arm study to evaluate the usefulness of ILR for detecting arrhythmia.
to 1828 msec. ) — which corresponds to a variation in the rate of sinus bradycardia from 36-to-33/minute. This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute.
There are three mechanisms of arrhythmia: automatic, re-entry, and triggered. The most common triggered arrhythmia is Torsades de Pointes. Automatic activity refers to enhanced pacemaking function (typically from a non sinus node source), for example atrial tachycardia. This has been discussed many times before on this blog.
I will leave more detailed rhythm discussion to the illustrious Dr. Ken Grauer below, but this use of calipers shows that the rhythm interpretation is: Sinus bradycardia with a competing (most likely junctional) rhythm. That is, until the 7th R wave which comes a little bit sooner than expected. CLICK HERE — for more on fusion beats.
== P EARL # 1: The easiest way to instantly enhance your arrhythmia interpretation skills is by using calipers. The cardiologist who does not regularly use calipers for interpretation of complex arrhythmias is a cardiologist who will miss the diagnosis on more than a few occasions. Using calipers will NOT slow you down.
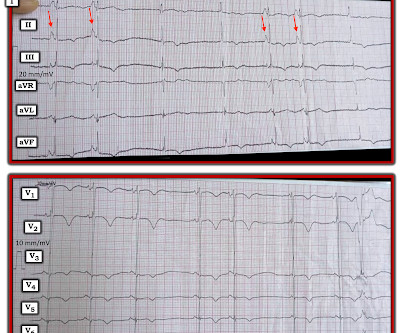
Looking first at the long-lead II rhythm strip — there is significant bradycardia , with a heart R ate just under 40/minute. The patient may need a pacemaker. But the point to emphasize — is that it should only take seconds to recognize that there is bradycardia from significant AV block. =
That said — obvious findings include: i ) Marked bradycardia! — My Immediate Impression — was that this elderly woman with a several week history of symptoms would most likely leave the hospital with a pacemaker. The rhythm in Figure-1 is complex — and defies precise interpretation without careful study. be regular! —
Reflex syncope is defined as a transient loss of consciousness due to a neurally mediated reflex causing sudden-onset vasodilation and bradycardia, leading to a steep decrease in blood pressure and cerebral hypoperfusion. Thus, once the aetiology is established, further diagnostic tests are seldom performed.
Isoprenalin was discontinued, and a temporary transveous pacemaker was implanted. The patient stabilized following pacemaker placement. VT is the second most common presenting arrhythmia. Vaso or inotropic medications are not harmless, and can precipitate life threatening arrhythmias.
Most of the time with AV block — the atrial rhythm will be regular ( or at least almost regular — if there is an underlying sinus arrhythmia ). PEARL # 5: As noted above — today's arrhythmia appears to represent some form of 2nd-degree AV block. Figure-4: I needed to draw a laddergram.
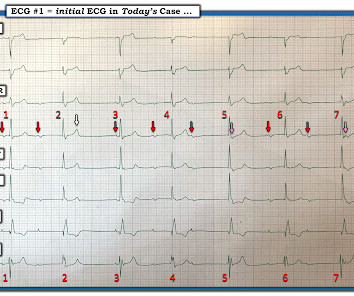
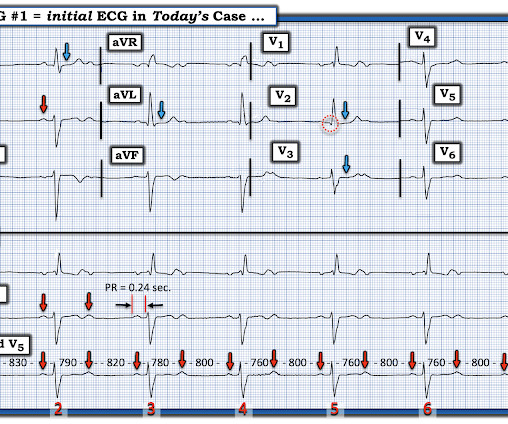
I added, "Makes me wonder if this could be myocarditis in a younger adult — maybe even with sinus arrhythmia." That said, despite the group beating — the rhythm is not consistent with AV Wenckebach. Figure-1: The initial ECG in today's case.
There are 3 etiologies I always think of with bradycardia and AV block: 1. She had a permanent pacemaker implanted. After pacer AND conversion to sinus rhythm: Computer diagnosis: IMPRESSION ELECTRONIC VENTRICULAR PACEMAKER ABNORMAL RHYTHM ECG What is missing from this interpretation? Hyperkalemia. Her K was normal 3.
Baseline bradycardia in endurance athletes limits the use of ß-blockers. The Role of Sinus Arrhythmia: I found it interesting to compare the long lead II rhythm strips in the 3 serial tracings from today’s case ( Figure-1 ). Note fairly marked irregularity of the R-R interval — indicative of definite sinus arrhythmia.
Arrhythmia In simple words, arrhythmia refers to an irregular heartbeat. A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. ECG testing is also carried out to see how medicines work during treatment and the pacemaker's functioning.
Athlete’s bradycardia due to increased parasympathetic tone and decreased sympathetic tone is a well-known observation. Though sinus bradycardia is usual, other abnormalities like sinus arrhythmia, sinus arrest, wandering atrial pacemaker and coronary sinus rhythm have been described.
He received a permanent pacemaker during the subsequent inpatient stay. plaque disruption), the T waves still manifest markings of a previous state of suboptimal coronary flow that resolved: Type II supply-demand mismatch in the setting of extreme bradycardia. Chapter 17: Ventricular Arrhythmias. References [1] Surawicz, B.
Therefore, she underwent temporary pacemaker placement and overdrive pacing at a rate of 90 bpm to keep the heart rate up in order to prevent these PVCs triggering ventricular arrhythmia. Hypokalemia was unlikely because she continued to have ventricular arrhythmia despite of correcting electrolytes.
To improve visualization — I've digitized the original ECG using PMcardio ) MY Thoughts on the ECG in Figure-1: This is a challenging tracing to interpret — because there is marked bradycardia with an irregular rhythm and a change in QRS morphology. Was there a family history of sudden death or significant arrhythmia?
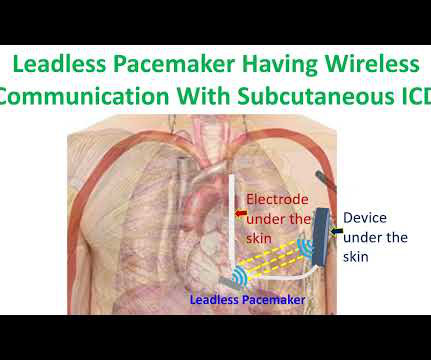
But subcutaneous ICD cannot provide bradycardia and antitachycardia pacing as a transvenous ICD. It was a multinational study which enrolled patients at risk for sudden death from ventricular arrhythmias and the follow up period was 6 months. of patients were free from leadless pacemaker related major complications.
PVCs N ot generally considered abnormal ECG findings: Isolated PAC, First Degree AV Block, Sinus bradycardia at a rate of 35-45, and Nonspecific ST-T abnormalities (even if different from a previous ECG). Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful.
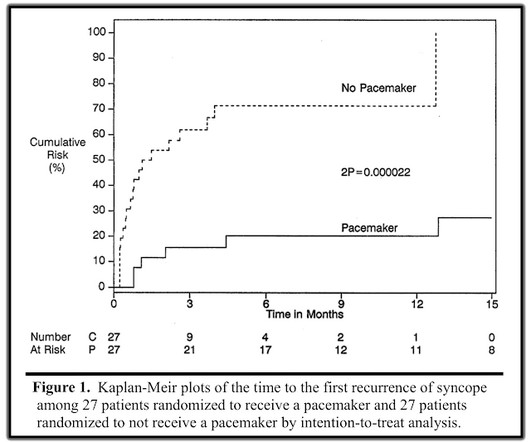
If the block is not vagal in nature, the patient should receive a pacemaker. There was a randomized trial to determine whether pacemakers could benefit patients with vasovagal syncope, aptly named The North American Vasovagal Pacemaker Study (VPS). In the repeat study (VPS II), EVERY patient had an implanted pacemaker.
To Emphasize: Regardless of whether the rhythm in Figure-1 represents 2nd- or 3rd-degree AV block — the overall ventricular rate is slow ( in the 40s/minute ) — so that IF this patient is symptomatic and no “fixable” cause of the bradycardia is found — pacing might still be needed. The "Longer" Answer: = What then is going on?
The patient went for EP study and had prolonged HV interval which strongly supports placement of a pacemaker. He underwent dual chamber pacemaker implantation and did well. What follows is a "deep dive" into some of the intricacies of the 2nd-degree AV block for readers with an interest in advanced arrhythmia interpretation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content