This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. Because she has cardiomyopathy and ventricular dysrhythmias, the pacer included an Implanted Cardioverter-Defibrillator (ICD) Echo 6 days later after CRT: Normal estimated left ventricular ejection fraction. The plan: 1.
Ventricular tachycardia is a potentially life threatening cardiac arrhythmia. Recurrent ventricular tachycardia in spite of radiofrequency catheter ablation needs an implantable cardioverter defibrillator. If the rate is very fast, hemodynamic deterioration can occur rapidly.
After resuscitation and defibrillation , there were no more episodes of TdP. Below is the patient’s 12 lead ECG following defibrillation. Learning points : Takotsubo can lead to cardiac arrest from ventricular arrhythmia. NT-proBNP was significantly elevated at 4900ng/L ( ref < 500ng/L ). What does this ECG tell you?
Similarly, you may use our , app to adjust the paper speed along with amplification to read the slightest changes, especially for conditions like tachycardia and bradycardia. Alternatively, it also helps enhance arrhythmia management with coronary artery disease. It improves the prediction model for myocardial scar mass.
We examined the effect of ibutilide, a class III antiarrhythmic agent, on the energy requirement for atrial defibrillation and assessed the value of this agent in facilitating cardioversion in patients with atrial fibrillation that is resistant to conventional transthoracic cardioversion. 25, 2022 ).
She was never defibrillated. Therefore, she underwent temporary pacemaker placement and overdrive pacing at a rate of 90 bpm to keep the heart rate up in order to prevent these PVCs triggering ventricular arrhythmia. Hypokalemia was unlikely because she continued to have ventricular arrhythmia despite of correcting electrolytes.
However, he suddenly developed a series of malignant ventricular arrhythmias. He required multiple defibrillations within a period of a few hours. Below are printouts of some of the arrhythmias recorded. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation.
Here is the transcript of the video: Implantable defibrillator is an important life saving device. It can automatically detect life threatening ventricular arrhythmias and treat them, either with a shock or, sometimes by overdrive pacing. These are high voltage, defibrillator shock coils. So, this is how an ICD works.
She was given CRT-D (Cardiac Resynchronization Therapy-Defibrillator). VT is the second most common presenting arrhythmia. Vaso or inotropic medications are not harmless, and can precipitate life threatening arrhythmias. It is common with 2nd- and 3rd-degree AV block to see a " ventriculophasic " sinus arrhythmia.
There is also bradycardia. Bradycardia puts patients at risk for "pause-dependent" Torsades de Pointes. Torsades in acquired long QT is much more likely in bradycardia because the QT interval following a long pause is longer still. malignant ventricular arrhythmias are present), rapid replacement of potassium is required.
The arrhythmia spontaneously converted before defibrillation was achieved. As per Dr. Nossen — today's initial ECG ( LEFT tracing in Figure-2 ) shows sinus bradycardia with QRS widening due to bifascicular block ( RBBB/LAHB ). Just prior to arrival he fell out of consciousness with the below ECG on the monitor.
The patient was put on Extracorporeal Life Support in the ED 3 hours after initial resuscitation, the core temp was 30° C and the patient was defibrillated with a single attempt. On arrival, CPR was continued and core temperature was measured at 18° C (64.4° A 12-lead ECG was recorded: There is sinus rhythm with RBBB and right axis deviation.
Prior to Mizusawa's study, it was thought that the incidence of syncope, arrhythmia, or SCD in this cohort was low [7]. In light of the risk of arrhythmia events observed in the Mizusawa trial, a formal EP study might be reasonable to obtain in those with fever induced asymptomatic Brugada ECG changes to help risk stratify these patients.
Cardioversion/defibrillation. Bradycardia. Finally — a detailed family history ( for early sudden death ) + a careful personal history ( for syncope/presyncope; malignant arrhythmia ) is in order. Acute febrile illness. Variations in autonomic tone. Hypothermia. Electrolyte imbalance ( hypokalemia; hyperkalemia ).
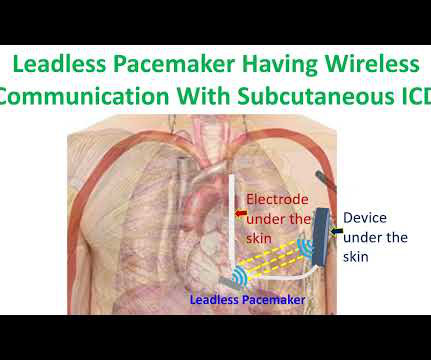
Subcutaneous implantable cardioverter defibrillator was an innovation meant to reduce the lead related problems of conventional transvenous ICDs. But subcutaneous ICD cannot provide bradycardia and antitachycardia pacing as a transvenous ICD. None of the deaths in the study were deemed to be arrhythmia related or procedure related.
Regardless of further evaluation, she should avoid bradycardia, AV nodal blockers, Na channel blockers, and fevers. --If Conclusion of this paper: Fever is a great risk factor for arrhythmia events in Brugada Syndrome patients. EP study to further risk stratify her is recommended, with ICD placement depending on the results.
The possibility of an ischemic cause of the ventricular arrhythmia has to be considered! Below in Figure-5 is a 10-minute continuous lead II recording on oral Flecainide, now showing sinus bradycardia without a single PVC! A workup was undertaken in search of a cause of the patient's ventricular arrhythmia. No PVCs are seen.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content