This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Notwithstanding many insightful observations, the electrocardiogram (ECG) arguably ignited the big bang in our understanding of cardiac arrhythmias. Using ECG recording and deductive reasoning, our teachers and predecessors classified the bradycardias and tachycardias and proposed many mechanisms, subsequently proven to be correct.
BackgroundThere have been few instances of symptomatic bradycardia-arrhythmia in the context of area postrema syndrome (APS), and some of them have been implanted permanent pacemakers. Brady-arrhythmia was presented in all patients, and 9 patients were implanted temporary or permanent pacemakers.
Sinus bradycardia – sinus rhythm below 60 bpm is a sinus bradycardia. Other times, an irregular recording can signal a medical emergency, such as a myocardial infarction or a dangerous arrhythmia. 1] Arrhythmia Recognition: The Art of Interpretation, T.Garcia, D.Garcia. Usually does not exceed 160 bpm.
The primary outcome was ventricular arrhythmias, the secondary outcomes were bradycardia and atrial fibrillation (AF).ResultsOur Perioperative or postoperative use of DEX reduced the incidence of in-hospital ventricular arrhythmias [Odds Ratio (OR) 0.14, 95% Confidence Interval (CI) 0.03–0.66], 8.17) compared with propofol.
For full discussion of the case — CLICK HERE — ECG Rhythm Overview: A 12-year-old boy was admitted to our hospital with severe myocardial dysfunction and chaotic rhythm with tachy- and bradycardic arrhythmias. There definitel are periods of bradycardia (so pacing may be needed for that).
Cardiac accumulation triggers local tissue injury, electrical instability and arrhythmia. Objective We conducted a systematic review evaluating AF burden and bradycardia requiring permanent pacemaker (PPM) implantation and report any predictive risk factors identified. Study outcomes included AF or bradycardia requiring therapy.
Krantz et al authored a State-of-the-Art Review on Cardiovascular Complications of Opioid Use ( JACC 77(2):205-223, 2021 ) — in which mechanisms from Opioid Overdose that detail arrhythmia production ( up to cardiac arrest ) are elucidated — thereby providing an explanation for the unusual arrhythmias in today's case.
With P waves labeled — Isn't it now much easier to appreciate that the atrial rhythm is quite regular ( with no more than a slight sinus arrhythmia )? P utting I t A ll T ogether : The precise mechanism of today's arrhythmia is complex and difficult to determine. For those with a special interest in cardiac arrhythmias — READ ON! —
Insertable cardiac monitors (ICMs) are used widely for long term monitoring and diagnosis of various cardiac arrhythmia. Among them, bradycardia and pause detection could be erroneous during sleep as the heart rate may slow down significantly leading to potential inappropriate diagnosis.
IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr. Smith's ECG Blog ). Initial high sensitivity troponin I returned at 6ng/L (normal 0.20
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. As described above by Dr. Smith Pacing in today's case is an effective intervention as doing so prevents the bradycardia and pauses that are likely to precipitate additional episodes of Torsades de Pointes. (
Altered Mental Status, Bradycardia == MY Comment , by K EN G RAUER, MD ( 2/2 /2024 ): == Dr. Meyers began today’s case with the clinical challenge of asking you to identify the underlying cause of ECG #2. -- Read this ECG -- Osborn Waves and Hypothermia (this is the "Figure" above) What does LBBB look like in severe hypothermia?
to 1828 msec. ) — which corresponds to a variation in the rate of sinus bradycardia from 36-to-33/minute. This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute.
Background The rising adoption of wearable technology increases the potential to identify arrhythmias. Those with arrhythmias or non-diagnostic EKGs were sent 7-day monitors. The EHR was reviewed after 3 years to determine if participants developed arrhythmias. Mean age was 50.5 (SD years, and 46 (53.3%) were female.
Learning objectives To review the potential arrhythmia complications during pregnancy and puerperium in women with and without known cardiovascular disease. To recognise arrhythmia conditions associated with a high risk of pregnancy-related cardiac complications for which intervention before considering pregnancy is appropriate.
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. Limiting one's interpretation to marked bradycardia with high-grade AV block in need of pacing in this patient with multiple syncopal epiosodes — more than suffices for "the quick answer". Figure-3: I've labeled ECG #3.
Abstract Background Programed ventricular stimulation (PVS) is a risk stratification tool in patients at risk for adverse arrhythmia outcomes. Patients with negative PVS may yet be at risk for adverse arrhythmia-related events, particularly in the presence of symptomatic ventricular arrhythmias (VA).
I will leave more detailed rhythm discussion to the illustrious Dr. Ken Grauer below, but this use of calipers shows that the rhythm interpretation is: Sinus bradycardia with a competing (most likely junctional) rhythm. preceding each of the fascicular beats — indicating a faster rate for the escape rhythm compared to the sinus bradycardia ).
during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. The easy way to remember the arrhythmias most commonly associated with SSS is to think of what one might expect if the SA node became sick. The indication for pacemaker placement with SSS is symptomatic bradycardia.
Early detection of conditions like AFib, bradycardia, or tachycardia allows patients to address issues before they become critical. Risk Reduction Data from wearables can identify potential risks, such as undiagnosed arrhythmias or hypertension, allowing healthcare teams to address these issues before surgery.
Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). NOTE: Prediction of cardiac contusion "severity" on the basis of cardiac arrhythmias and ECG findings — is an imperfect science. RBBB in blunt chest trauma seems to be indicative of several RV injury. QTc prolongation.
Other cardiac-related causes for syncope associated with acute MI may include malignant ventricular arrhythmias and bradyarrhythmias including AV block. The "good news" — is that a cardiac-related cause of syncope is unlikely if the initial ECG is normal, and cardiac monitoring in the ED fails to reveal significant arrhythmia.
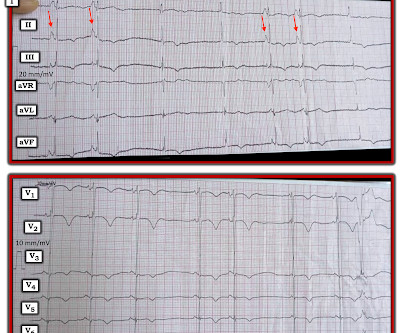
Looking first at the long-lead II rhythm strip — there is significant bradycardia , with a heart R ate just under 40/minute. But the point to emphasize — is that it should only take seconds to recognize that there is bradycardia from significant AV block. = Would you approve her for a nonemergent surgical procedure?
== P EARL # 1: The easiest way to instantly enhance your arrhythmia interpretation skills is by using calipers. The cardiologist who does not regularly use calipers for interpretation of complex arrhythmias is a cardiologist who will miss the diagnosis on more than a few occasions. Using calipers will NOT slow you down.
Whatever the specific etiology of today's arrhythmia is, the “good news” is — that this rhythm will most probably improve with reperfusion of the "culprit" artery. That said — I found today's arrhythmia fascinating, and worthy of more in-depth analysis. Using calipers facilitates the process.
Most of the time with AV block — the atrial rhythm will be regular ( or at least almost regular — if there is an underlying sinus arrhythmia ). PEARL # 5: As noted above — today's arrhythmia appears to represent some form of 2nd-degree AV block. Figure-4: I needed to draw a laddergram.
That said — obvious findings include: i ) Marked bradycardia! — L addergram I llustration : At this point — I needed to work out, and then draw a laddergram that I could then verify to ensure a plausible mechanism for today's arrhythmia. The rhythm in Figure-1 is complex — and defies precise interpretation without careful study.
Ventricular tachycardia is a potentially life threatening cardiac arrhythmia. Polymorphic VT is managed by intravenous magnesium and measures to increase heart rate like pacing as it occurs most often in the setting of bradycardia and QT interval prolongation. If the rate is very fast, hemodynamic deterioration can occur rapidly.
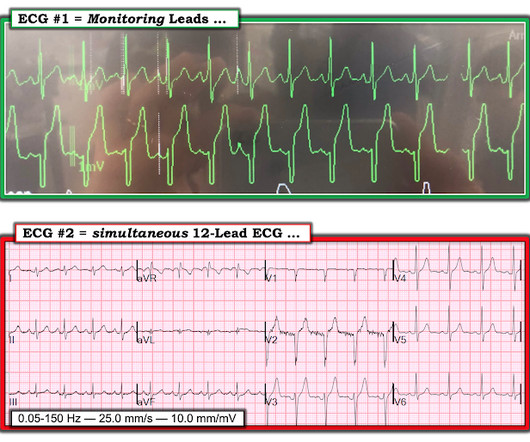
I added, "Makes me wonder if this could be myocarditis in a younger adult — maybe even with sinus arrhythmia." That said, despite the group beating — the rhythm is not consistent with AV Wenckebach. Figure-1: The initial ECG in today's case.
KEY Point: Knowing that the most commonly overlooked arrhythmia is AFlutter — suggests that the BEST way to avoid missing the diagnosis of AFlutter is simply to THINK of AFlutter whenever you have a regular SVT at a rate close to 150/minute ( in which you do not clearly see upright sinus P waves in lead II ).
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. Serious AEs were rare; 1 patient in the etripamil arm experienced transient severe bradycardia and syncope, assessed as due to hyper-vagotonia.Conclusions:Intranasal etripamil 70 mg reduced VR and improved symptom-relief and treatment-satisfaction.
I focus my comments purely on a few sophisticated concepts in arrhythmia recognition — fully aware that specific rhythm disorders with calcium channel toxicity need not be treated per se, beyond providing cardiovascular support. It's always rewarding and mutually educational to discuss interesting aspects of arrhythmia interpretation.
Baseline bradycardia in endurance athletes limits the use of ß-blockers. The Role of Sinus Arrhythmia: I found it interesting to compare the long lead II rhythm strips in the 3 serial tracings from today’s case ( Figure-1 ). Note fairly marked irregularity of the R-R interval — indicative of definite sinus arrhythmia.
Learning points : Takotsubo can lead to cardiac arrest from ventricular arrhythmia. Most Torsades is the result of a pause-dependent effect that predisposes to development of the malignant arrhythmia ( Dohadwala et al — Heart Rhythm Case Rep 3(2):115-119, 2017 ).
Similarly, you may use our , app to adjust the paper speed along with amplification to read the slightest changes, especially for conditions like tachycardia and bradycardia. Alternatively, it also helps enhance arrhythmia management with coronary artery disease. It improves the prediction model for myocardial scar mass.
He has a family history concerning for arrhythmia. Given the circumstances of his car crash, we presume it was due to an underlying arrhythmia. He has a family history concerning for arrhythmia with his father requiring some sort of device (PPM, ICD, unclear) at a young age.
The computer called "Sinus Bradycardia" only (implying that everything else is normal. The overreading Cardiologist called it only "Sinus Bradycardia" with no other findings. The rhythm in Figure-1 is sinus bradycardia and arrhythmia. These features are subtle — but they are definitely present and important to recognize.
Athlete’s bradycardia due to increased parasympathetic tone and decreased sympathetic tone is a well-known observation. Though sinus bradycardia is usual, other abnormalities like sinus arrhythmia, sinus arrest, wandering atrial pacemaker and coronary sinus rhythm have been described.
Cardiology was consulted, and the note said "no arrhythmias on telemetry or pacer interrogation." This is supported by the PT note which described a palpably irregular pulse with pauses and marked bradycardia. The final cardiology recommendation was to increase fludrocortisone and midodrine.
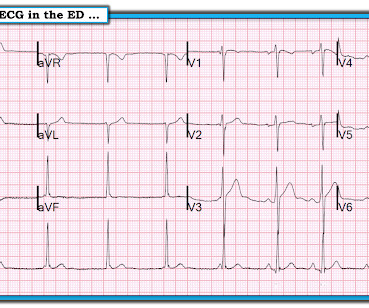
The ECG shows sinus bradycardia but is otherwise normal. Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." The documentation does not describe any additional details of the history. The following ECG was obtained. ECG 1 What do you think?
There are 3 etiologies I always think of with bradycardia and AV block: 1. While the diagnosis of SSS may become readily apparent early on in many patients clear indication for pacing usually does not become established until there is profound, symptomatic bradycardia usually requiring pauses of at least 3.0 Hyperkalemia.
Instead — my thoughts were as follows: The rhythm is sinus , with marked bradycardia and a component of sinus arrhythmia. WPW Cardiac arrhythmias ( especially AFib ). Smith's — in that despite the alarming ST-T wave changes, I did not think ECG #1 was the result of an acute event. Abnormal ST-T wave abnormalities.
Additionally, his cardiac telemetry monitor showed runs of accelerated idioventricular rhythm, a benign arrhythmia often associated with coronary reperfusion. He had multiple episodes of bradycardia and nonsustained ventricular tachycardia. As expected, the patient reported total resolution of pain by the time he got to the ED.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content