This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Atrialfibrillation is the most prevalent arrhythmia with a lifetime risk of nearly 30%. Pulmonary vein isolation (PVI) is the most effective treatment for rhythm control. It can be associated with reduced quality of life and complications such as heart failure and stroke.
Based on continuous monitoring of early recurrence of atrial tachyarrhythmia immediately after patients have undergone atrialfibrillation ablation, Musat et al. However, this reasoning disregards valuable data regarding early arrhythmia recurrences and their potential significance.
Specific cardiovascular diseases, such as acute myocardial infarction, arrhythmias, pulmonary hypertension and pericarditis, were also pointed. Elevated risk of arrhythmias, particularly atrialfibrillation, correlated with occupational silica exposure.
Unlike paroxysmal AF, which describes symptoms that last for seven days or fewer, persistent AF is a sustained arrhythmia that lasts for more than a week 1. Early treatment of persistent AF can reduce the risk of blood clots, stroke, and heart failure, and may prevent the disease from becoming permanent.
Both atria develop from a combination of the primitive atrium, sinus venous, and pulmonary veins.It When atrialfibrillation (AF) begins, it can start with a single focus, degenerating to multiple wavelets, and it spreads throughout the entire surface area of both atria. The baseline RA dimension is a few mm more than LA.
Current guideline indications for intervention in asymptomatic patient are centred on left ventricular dimensions and ejection fraction and may include consideration in atrialfibrillation, pulmonary hypertension and those with left atrial dilatation.
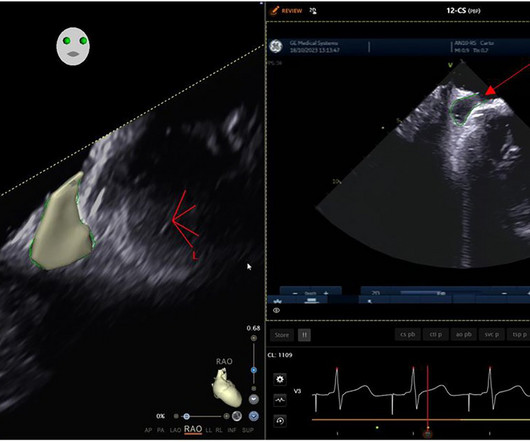
Whilst pulmonary vein isolation (PVI) is the key endpoint for catheter ablation therapy for atrialfibrillation (AF), it is unknown whether adjunctive carinal ablation impacts outcome beyond achieving first pass isolation.
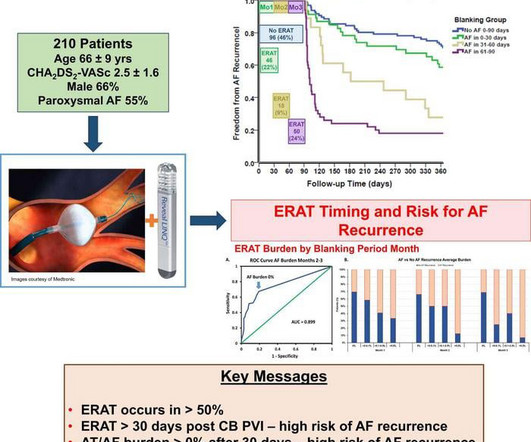
Despite advances in treatment of atrialfibrillation (AF) with pulmonary vein isolation (PVI), AF recurrence remains a challenge. High tx burden pre-PVI may lead to difficulty maintaining arrhythmia freedom post-PVI.
At present we do not have any reliable intra-procedural electrophysiologic predictors of long-term success of AF ablation other than pulmonary vein isolation. We evaluated selected intraprocedural pulmonary vein characteristics that may be helpful in future guidance of persistent AF ablation. Results PV capture was identified in 20.3%
Atrialfibrillation (AF) is the most common sustained cardiac arrhythmia in adults, leading to significant cardiovascular complications such as ischemic stroke, heart failure, and myocardial infarction. Pulmonary vein isolation (PVI) is a well-established treatment for rhythm control in patients with AF.
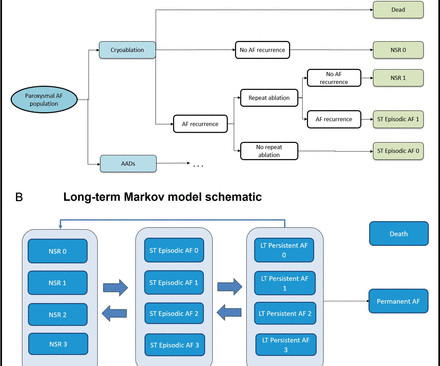
Introduction Three recent randomised controlled trials have demonstrated that pulmonary vein isolation as an initial rhythm control strategy with cryoablation reduces atrialarrhythmia recurrence in patients with symptomatic paroxysmal atrialfibrillation (PAF) compared with antiarrhythmic drug (AAD) therapy.
Background Pulmonary vein isolation with wide antral ablation leads to better clinical outcomes for the treatment of atrialfibrillation, but the isolation lesion is invisible in conventional cryoballoon ablation. The rate of 12-month freedom from clinical atrialarrhythmia recurrence was 85.1%
Animal studies suggest that catheter ablation-associated parasympathetic and sympathetic denervation could result in increased ventricular arrhythmias (VA). The impact of catheter ablation of atrialfibrillation on VA burden in humans has not been assessed.
Catheter ablation via pulmonary vein isolation (PVI) is first-line treatment for paroxysmal atrialfibrillation (pAF). It is unclear whether additional lesions with PVI using the novel pulsed field ablation (PFA) technique affects outcomes in this population.
Persistent atrialfibrillation (AF) ablation targeting extra-pulmonary vein drivers using various technologies has delivered varying results from no benefit to significant arrhythmia free survival.
Pulmonary vein isolation (PVI) is an effective treatment for atrialfibrillation (AF). Baseline heart rate (HR) in normal sinus rhythm (NSR) has been observed to increase after PVI, thought to be due to modification of ganglionated plexi during PVI.
Overview of the study population and effects observed after catheter ablation for atrialfibrillation. PVI, pulmonary vein isolation. Herein we describe the effects of catheter ablation on AF burden, arrhythmia recurrences, and ventricular function in end-stage HF. Median AF burden reduction was 36.3
Pulsed field ablation (PFA) is a promising new alternative to thermal ablation (TA) for atrialfibrillation (AF), improving safety and duration of procedure times. While pulmonary vein isolation (PVI) durability appears comparable between PFA and TA, the necessity of post-ablation remapping remains uncertain.
Multiple randomized controlled trials (RCTs) have compared the efficacy of pulmonary vein isolation (PVI) adjunctive techniques with PVI alone in patients with persistent atrialfibrillation (AF).
Background Catheter ablation (CA) for symptomatic atrialfibrillation (AF) offers the best outcomes for patients. We present real-world 5-year follow-up data of AI-guided pulmonary vein isolation. We present real-world 5-year follow-up data of AI-guided pulmonary vein isolation. Age >75 years ( p = 0.02, HR: 2.7,
Since pulmonary vein isolation (PVI)the standard treatment for atrialfibrillation (AF)is inadequate for persistent AF (PsAF), various extra-PVI strategies have been proposed.
a global leader in cardiac arrhythmia treatment and part of Johnson & Johnson MedTechi , revealed findings from a company-funded study of real-world data. AFib is the most common type of cardiac arrhythmia and affects more than 6 million people in the United States and nearly 38 million people worldwide.2,3 In: AF Symposium.;
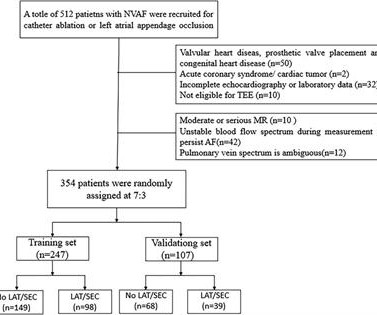
Background Atrialfibrillation (AF) is the most common cardiac arrhythmia and is associated with a high risk of stroke. Conclusion Our findings indicate that an enlarged left atrium and abnormal hemodynamic parameters in the left atrial and pulmonary veins are linked to a greater risk of LAT/SEC.
Backgroundwide antral pulmonary vein isolation (PVI) is effective for treating paroxysmal atrialfibrillation (PAF), although time-demanding. The primary endpoint was achieved by 9% and 12% of cases at 12 and 24 month follow up, respectively.
Low voltage area (LVA) and low conduction velocity (CV) are promising risk factors to identify patients with abnormal atrial substrate at a high risk of atrialfibrillation (AF) recurrence following pulmonary vein isolation (PVI).
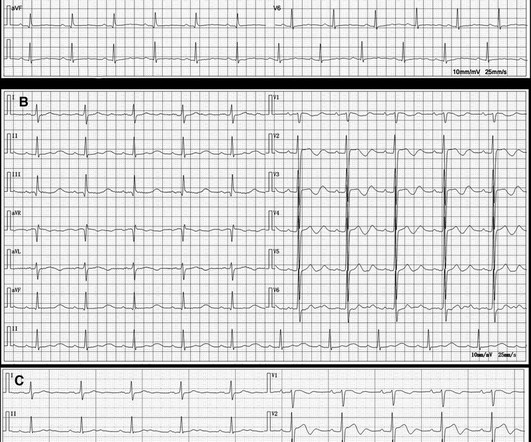
Here is the computer interpretation: ATRIALFIBRILLATION WITH RAPID VENTRICULAR RESPONSE WITH ABERRANT CONDUCTION OR VENTRICULAR PREMATURE COMPLEXES LEFT AXIS DEVIATION [QRS AXIS beyone -30] NONSPECIFIC ST and T-WAVE ABNORMALITY The over-reading physician confirmed this diagnosis, which is incorrect. It is not atrialfibrillation.
ABSTRACT Background Ultra-low temperature cryoablation (ULTC) is a technique designed to rapidly cool cardiac tissue to extremely low temperatures, enabling the creation of ablation lesions for the treatment of atrialfibrillation (AF). Arrhythmia outcomes after repeat ablation were evaluated.
Radiofrequency catheter ablation (RFCA) for persistent atrialfibrillation (AF) is associated with suboptimal long-term outcomes. Although increasing evidence supports substrate-based ablation strategies targeting extra-PV sources, reliable endpoints during CA beyond pulmonary vein (PV) isolation are not well established.
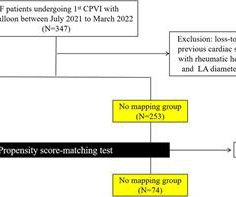
The Kaplan-Meier curve of all-atrialarrhythmia-free survival for (A) all persistent patients and (B) patients who underwent PSM conducted to the higher recurrence rate in PVI + group. Methods Data from early commercial use across seven European centers were collected in a registry. Procedural and follow-up data were collected.
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. BACKGROUND:Pulmonary vein isolation (PVI) alone is less effective in patients with persistent atrialfibrillation (AF) compared with those with paroxysmal AF. to 3.4%]; hazard ratio, 0.66 [95% CI, 0.460.94]).
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. BACKGROUND:High-power short-duration ablation has shown impressive efficacy and safety for pulmonary vein isolation (PVI); however, initial efficacy results with very high power short-duration ablation were discouraging. ie, noninferiority is met).
The first procedures were performed by Dr. David Newton , Clinical Cardiac Electrophysiologist at Memorial Health University Physicians Heart Care and Dr. Andrea Natale , Executive Medical Director at T exas Cardiac Arrhythmia Institute, St. David’s Medical Center.
This study of 16 patients with persistent left superior vena cava (PLSVC) undergoing atrialfibrillation ablation shows a 66.7% Abstract Objectives To investigate tailored approaches, techniques, and outcomes of catheter ablation in patients with persistent left superior vena cava (PLSVC) undergoing atrialfibrillation (AF) ablation.
Catheter ablation for atrialfibrillation (AF) aims to achieve durable pulmonary vein isolation (PVI) by creating transmural lesions that disrupt arrhythmogenic pathways. However, consistent and lasting success remains challenging due to variability in lesion formation and durability, contributing to arrhythmia recurrence.
Large footprint pulse field ablation (PFA) catheters have been widely adopted for pulmonary vein isolation (PVI) and posterior wall isolation (PWI) for atrialfibrillation. The role of large footprint PFA catheters for linear ablation in the treatment of organized atrialarrhythmias has not been well described.
Abstract Introduction Earlier studies have shown a clear association between severity of human immunodeficiency virus (HIV) infection and incident atrialfibrillation (AF). During first procedure, all received isolation of pulmonary vein (PV) + posterior wall and superior vena cava. vs. 87.1%, p = .753]
2 BB area pacing defined using P-wave criteria has been associated with decreased atrialarrhythmia burden, recurrence, and de novo incidence compared with right atrial septal pacing and right atrial appendage pacing.3
Although the QDOT MICRO™ Catheter was mainly designed for pulmonary vein isolation (PVI) its versatility to treat atrialfibrillation (AF) and other types of arrhythmias was recently evaluated by the FAST and FURIOUS study series and other studies and will be presented in this article.
Pulmonary vein isolation (PVI) has been established as a cornerstone therapy for atrialfibrillation (AF). Despite its effectiveness, over 20% of patients still experience recurrences of AF and atrial tachyarrhythmias (ATs) after PVI.1
The role of the right atrium (RA) in atrialfibrillation (AF) has long been overlooked. Multiple studies have examined clinical conditions associated with AF, such as atrial enlargement, fibrosis extent, electrical remodeling, and wall thickening, but have been mainly concentrated on the left atrium (LA).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content