This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Primary endpoint was the incidence of patients with new onset supraventricular arrhythmia (AF, atrial flutter or any supraventricular tachycardia) lasting >30s, post PFO closure.ResultsA total of 59 patients met the inclusion criteria. A total of 88 supraventricular arrhythmia events (96.6% days (IQR 1321).
For the past four decades, implantable cardioverter defibrillator (ICD) therapy has become the standard of care for preventing sudden cardiac death in high-risk individuals. The rate of ICD implantation has risen due to the increasing population age and the growing prevalence of cardiac arrhythmias.
BackgroundScreening for atrialfibrillation (AF) may reveal incidental arrhythmias of relevance. We furthermore report treatment decisions because of incidental arrhythmias. We found incidental arrhythmias in 94 patients (11.8%). Journal of the American Heart Association, Ahead of Print. of our cohort patients.
The wearable cardioverter defibrillator (WCD) is becoming a more and more widely used instrument for the prevention of sudden cardiac death of patients either with a secondary prevention implantable cardioverter defibrillator indication or with a transient high risk of sudden cardiac death.
Her Apple Watch suddenly told her that she is in atrialfibrillation. Patients with healthy AV nodes who are not on AV nodal blockers and who are not hyperkalemic should have a rapid ventricular response if they have paroxysmal Atrialfibrillation. Exam was completely normal except for an irregular heart rate.
The most common arrhythmia, atrialfibrillation , will affect approximately 12.1 Pacemakers and implantable cardioverter defibrillators (ICDs) are the standard of care to regulate a patient’s irregular heartbeat. UC San Diego Health implanted the pacemaker system in the first patient in February 2024. “To
“Therefore, we have made the decision to offer only DX technology for new patients needing a single-chamber ICD, providing equivalent therapies along with additional atrial monitoring data, as recommended by current guidelines.” For more information: [link] References: Thomas G, Choi DY, Doppalapudi H, et al. Margolis G, et al.
Abstract Introduction Wearable cardioverter defibrillator (WCD) is utilized in patients with assumed but not yet confirmed risk for sudden cardiac death (SCD). Many of these patients also present with atrialfibrillation (AF). events per 100 patient-years vs. 74.8 events per 100 patient-years, p < .001).
We conducted this systematic review and meta-analysis to evaluate safety outcomes including risk of ventricular arrhythmias, new onset atrialfibrillation, Implantable Cardiac defibrillators (ICD) shocks, QRS duration reduction, heart failure hospitalizations and mortality.
An interesting fact is that many of the persons experience arrhythmias in Brugada syndrome with fever. So there is some relation between fever and precipitation of arrhythmias in Brugada syndrome. Of course, the commonest sustained arrhythmia in general population is atrialfibrillation.
She was successfully revived after several rounds of ACLS including defibrillation and amiodarone. T-wave alternans and the susceptibility to ventricular arrhythmias. Chronic amiodarone evokes no torsade de pointes arrhythmias despite QT lengthening in an animal model of acquired long-QT syndrome. Pacing Clin Electrophysiol.
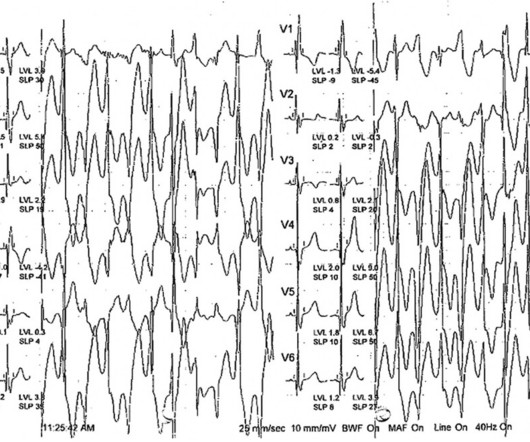
This can initiate ventricular arrhythmias like polymorphic ventricular tachycardia (PMVT). She was externally defibrillated with 200J and received magnesium and an IV amiodarone bolus. She was successfully defibrillated with 360J. Telemetry showed Spike-on-T phenomenon which initiated PMVT.
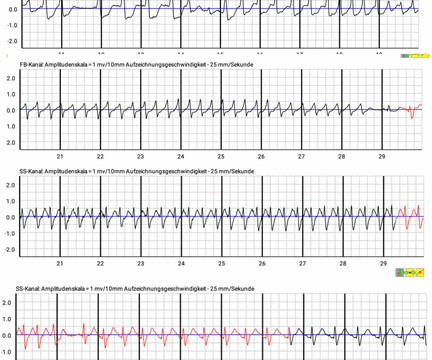
Note: Due to the limited number of normally conducted beats — it is hard to be sure whether the underlying rhythm is sinus with baseline artefact or atrialfibrillation. After resuscitation and defibrillation , there were no more episodes of TdP. Below is the patient’s 12 lead ECG following defibrillation.
The rhythm now is atrialfibrillation. The arrhythmia spontaneously converted before defibrillation was achieved. A repeat ECG was recorded about 15 minutes after the initial ECG. What do you think has happened and what is the most likely diagnosis? ECG #2 Again there is a wide complex QRS due to RBBB and LAFB.
The disorder is rare — but it takes on importance as a potential cause of atrial and ventricular arrhythmias, including cardiac arrest. Treatment is by ICD ( implantable cardioverter defibrillator ). SQTS is a relatively new diagnosis that has only been recognized as a distinct clinical entity since 2000.
The patient was put on Extracorporeal Life Support in the ED 3 hours after initial resuscitation, the core temp was 30° C and the patient was defibrillated with a single attempt. On arrival, CPR was continued and core temperature was measured at 18° C (64.4° A 12-lead ECG was recorded: There is sinus rhythm with RBBB and right axis deviation.
At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. There is atrialfibrillation. malignant ventricular arrhythmias are present), rapid replacement of potassium is required. Mean peak [K] p was 3.5
BackgroundCatecholaminergic polymorphic ventricular tachycardia (CPVT) is a rare inherited arrhythmia disorder characterized by ventricular arrhythmia triggered by adrenergic stimulation.Case presentationA 9-year-old boy presented with convulsions following physical exertion. High dose nadolol was required and amiodarone was added.
This causes deadly arrhythmias and should be considered in patients with syncope and short QT 2. The disorder is rare — but it takes on importance as a potential cause of atrial and ventricular arrhythmias, including cardiac arrest. Treatment is by ICD ( implantable cardioverter defibrillator ). Short QT syndrome.
Here is a representative CXR from a different patient showing a typical CRT-D The blue dotted line overlies the right atrial lead The red dotted line overlies the RV lead. This is the shock coil and identifies this device as a defibrillator. CRT-D is cardiac resynchronization therapy with defibrillation capability, like the CXR above.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content