This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
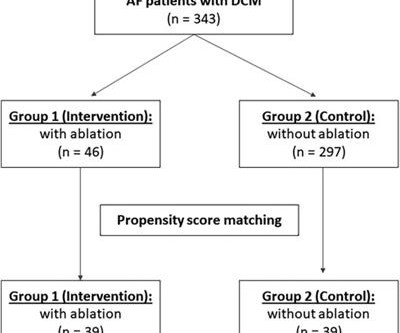
Introduction Catheter ablation is an effective and safe strategy for treating atrialfibrillation patients. Nevertheless, studies on the long-term outcomes of catheter ablation in patients with dilated cardiomyopathy are limited. Among the catheter ablation group, 58.7% ( n = 27) had persistent atrialfibrillation.
BackgroundAtrial fibrillation (AF) is the most prevalent cardiac arrhythmia worldwide, posing significant health burdens. Pulsed field ablation (PFA) is an emerging non-thermal technique that is gaining traction due to the ability to selectively target myocardial cells and minimize damage to surrounding tissues.
When atrialfibrillation (AF) begins, it can start with a single focus, degenerating to multiple wavelets, and it spreads throughout the entire surface area of both atria. A fibrillatory wave that occurs at a rate of more than 600 beats per minute can cause fatigue in the long run, leading to atrial dilation.
In this weeks View, Dr. Eagle looks at arrhythmia recurrence and rhythm control after catheter ablation for atrialfibrillation. He then discusses long-term outcomes in transthyretin amyloid cardiomyopathy in patients treated with tafamidis.
A gradual increase in arrhythmia recurrences during 12 months after catheter ablation (CA) of atrialfibrillation (AF) is still reported.1 A gradual increase in arrhythmia recurrences during 12 months after catheter ablation (CA) of atrialfibrillation (AF) is still reported.1
Catheter ablation of atrialfibrillation in infiltrative cardiomyopathies ABSTRACT Atrial and ventricular arrhythmias are common in patients with Infiltrative heart diseases. AF is the most common arrhythmia identified in patients with amyloidosis due to cellular infiltration and atrial dilation.
Development of a machine learning model to predict new-onset atrialfibrillation in patients with hypertrophic cardiomyopathy. Aims Atrialfibrillation (AF) is the most common sustained arrhythmia among patients with hypertrophic cardiomyopathy (HCM), leading to increased symptom burden and risk of thromboembolism.
Overview of the study population and effects observed after catheter ablation for atrialfibrillation. Herein we describe the effects of catheter ablation on AF burden, arrhythmia recurrences, and ventricular function in end-stage HF. PVI, pulmonary vein isolation.
Wild-type transthyretin amyloid cardiomyopathy (ATTRwt-CM) is often accompanied by atrialfibrillation (AF), atrial flutter (AFL), and atrial tachycardia (AT), which are difficult to control because beta-blockers and antiarrhythmic drugs can worsen heart failure (HF).
Long-term follow-up (FU) of the TRED-HF trial: persistent high-risk of relapse following therapy withdrawal in recovered dilated cardiomyopathy (DCM), likely contributed to by low-dose therapy and exposure to external triggers. LVEF, left ventricular ejection fraction. This follow-up investigates the longer-term effects of therapy withdrawal.
ABSTRACT Background Atrialfibrillation and atrial flutter are relatively rare in young people and the incidence of thromboembolic complications is unknown. Structural heart disease (SHD) was present in 120 patients (57%) and 20 patients (10%) had a primary cardiomyopathy.
Atrialfibrillation (AF), a common cardiac arrhythmia, often results in significant atrial remodeling, including atrialcardiomyopathy and dilatation. Notably, aFMR is linked to a higher recurrence rate of AF after catheter ablation.
Cardiac amyloidosis (CA) involves the abnormal accumulation of misfolded proteins in the heart muscle, leading to restrictive cardiomyopathy.1 Atrialarrhythmias (AA), particularly atrialfibrillation (AF), are prevalent in CA and may impact long-term cardiovascular outcomes, prompting an investigation into early rhythm management strategies.2
In this week’s View, Dr. Eagle looks at anticoagulation for post-operative atrialfibrillation after isolated coronary artery bypass grafting. He then examines a meta-analysis of invasive vs. conservative management of non-ST-elevation acute coronary syndromes with previous coronary artery bypass grafting.
The EHRA/HRS/APHRS/SOLAECE Expert Consensus on AtrialCardiomyopathies published in 2017 defined atrialcardiomyopathy as “any complex of structural, architectural, contractile, or electrophysiological changes affecting the atria.”1
Circulation: Arrhythmia and Electrophysiology, Ahead of Print. Atrialcardiomyopathy is a condition that causes electrical and contractile dysfunction of the atria, often along with structural and functional changes.
She was found to have atrialfibrillation and flutter with RVR. She underwent a cesarean section at 32 weeks given ongoing arrhythmia and heart failure symptoms. Her arrhythmia burden continued to lessen. Cardiomyopathy and arrhythmia have been described in a small number of cases.
ABSTRACT Atrialfibrillation (AF) is the most common cause of arrhythmia-induced cardiomyopathy. Effective management strategies include medical therapy for rate and rhythm control, catheter ablation (CA), and goal-directed medical therapy.
Circulation: Arrhythmia and Electrophysiology, Volume 16, Issue 11 , Page e012191, November 1, 2023. BACKGROUND:The cause of hypertrophic cardiomyopathy (HCM) in the young is highly varied. Six (21%) patients had clinical atrialfibrillation (1 with shortest preexcited RR interval <250 ms).
Hypertrophic cardiomyopathy is a genetic disorder with a guarded prognosis which occurs in about 1:500 individuals. The most common symptom of hypertrophic cardiomyopathy is dyspnoea which occurs in 90% of cases and is due to elevated left ventricular diastolic pressures as a consequence of the diastolic dysfunction.
Studies have shown that mutations in the RYR2 gene, which encodes the RyR2 protein, are linked to several cardiac arrhythmias, including catecholaminergic polymorphic ventricular tachycardia (CPVT), long QT syndrome (LQTS), calcium release deficiency syndrome (CRDS), and atrialfibrillation (AF).
The advent of transseptal puncture has enabled the study of atrialfibrillation mechanisms, while epicardial access has enabled exploration of the epicardium in ventricular arrhythmias (ventricular tachycardia/ventricular fibrillation [VF]).1,2
T-wave alternans and the susceptibility to ventricular arrhythmias. Chronic amiodarone evokes no torsade de pointes arrhythmias despite QT lengthening in an animal model of acquired long-QT syndrome. Both ST segment and T wave alternans have been known to precede malignant ventricular arrhythmias. Pacing Clin Electrophysiol.
Note: Due to the limited number of normally conducted beats — it is hard to be sure whether the underlying rhythm is sinus with baseline artefact or atrialfibrillation. Note: The patient while on telemetry had alternating atrialfibrillation, sinus rhythm with 1st degree AV block and also periods of Wenckebach conduction.
It is dangerous in WPW with atrialfibrillation. In AtrialFibrillation, the tachycardia will always be irregularly irregular. In my opinion — it is a mistake to interpret arrhythmias in strict "binary" fashion — since rather than "either/or" — optimal interpretation is more of a probability statement.
Logistic regression was used to analyze the relationship between the treatment groups and hospital readmission within 90 days.Results:Only 517 AA met inclusion criteria and did not meet exclusion criteria, which included a history of valvular heart disease, hypertrophic or restrictive cardiomyopathy, active myocarditis, history of cardiac arrest, and (..)
She also has a hx of paroxysmal atrialfibrillation and is on oral anticoagulant treatment. There is almost always the possibility of exceptions ( ie, prior infarction or cardiomyopathy that might result in a very abnormal baseline tracing ). The last echocardiography 12 months ago showed HFmrEF.
They had a history of non-ischemic cardiomyopathy (EF 30%), as well as PCI with one stent. Detail of Flutter waves The rate of the flutter waves matches the rate of the WCT (about 200/m), proving that the presenting WCT had been 1:1 atrial flutter. The subsequent EP study could not induce VT, only atrialfibrillation.
He had a h/o ischemic cardiomyopathy and right MCA stroke. He was brought to the critical care area where these rhythms were seen on the monitor: Wide complex tachycardia with no apparent P-waves, and very irregular Consistent with atrialfibrillation with aberrancy A Regular wide complex tachycardia.
Both ST segment and T wave alternans have been known to precede malignant ventricular arrhythmias. Conduction and refractoriness alternans may be seen with WPW-related as well as AV Nodal-dependent reentr y tachycardias — atrialfibrillation — acute pulmonary embolus — myocardial contusion — and severe LV dysfunction.
Cardiomyopathies: These diseases affect the heart muscle, impairing its ability to pump blood effectively. Mutations in specific genes often cause hypertrophic cardiomyopathy and dilated cardiomyopathy.
Introduction Danon disease is an X-linked disorder caused by pathogenic variants in lysosome-associated membrane protein 2 ( LAMP2 ) gene, typically characterized by the triad of hypertrophic cardiomyopathy, myopathy, and intellectual disability. However, many patients may not present the typical presentation, especially in the early stage.
By 1909 ECGs were being used to diagnose cases of arrhythmia; by 1910 to diagnose indicators of a heart attack. to develop an AI-algorithm for identifying and triaging patients with Hypertrophic cardiomyopathy (HCM), a condition currently undetected in 80% of cases.
Background:Obstructive sleep apnoea (OSA) is highly prevalent in patients with obstructive hypertrophic cardiomyopathy (oHCM), and the severity of OSA appears to worsen following septal myoectomy. vs. 27.77 ± 3.26, p<0.001), a higher proportion of atrialfibrillation, hypertension, and history of smoking.
Introduction Apical hypertrophic cardiomyopathy (ApHCM) is a subtype of hypertrophic cardiomyopathy (HCM) that affects up to 25% of Asian patients and is not as well understood in non-Asian patients.
Updated Mayo Clinic HCM Genotype Predictor Score: Iuri Ferreira Felix, MD (USA) presented the updated Mayo Clinic HCM Genotype Predictor Score, a valuable screening tool for identifying hypertrophic cardiomyopathy (HCM) patients with a high likelihood of testing positive for genetic mutations. Read the published study.
AtrialFibrillationAtrialfibrillation causes irregular heartbeat, and the heart's normal blood supply is affected. Since atrialfibrillation can also be intermittent, such patients should continuously monitor their heart activity while performing daily activities with a portable ECG device.
The absence of any wall motion abnormality makes ischemic cardiomyopathy very unlikely. The new onset cardiomyopathy was thought to be due to both drug/alcohol use and to Tachycardia-Induced Cardiomyopathy. after atrial surgery • Not stopped by adenosine (0/13 pts, incl. Mild to moderate mitral regurgitation.
The primary outcome was a composite of all-cause death, heart failure, atrialfibrillation, ventricular arrhythmias, myocardial infarction, and Takotsubo cardiomyopathy 30 days from the stroke. 1.34]), atrialfibrillation (HR, 1.11 [95% CI, 1.09–1.13]), 1.13]), ventricular arrhythmias (HR, 1.38 [95% CI, 1.30–1.46]),
Atrail electroanatomic voltage mapping (Atrial-EAVM) and late gadolinium enhancement imaging (Atrial-LGE) quantify the functional and anatomic extent of atrial fibrosis, a central component of atrialcardiomyopathy. Atrial-EAVM and Atrial-LGE correlated with greatest agreement at high-fibrosis burdens.
BackgroundHypertrophic cardiomyopathy (HCM) is characterized by an increased left ventricular (LV) wall thickness and LV mass. Typical symptoms associated with HCM include atrialfibrillation (AF), syncope, ventricular fibrillation, and cardiac arrest.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content