This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
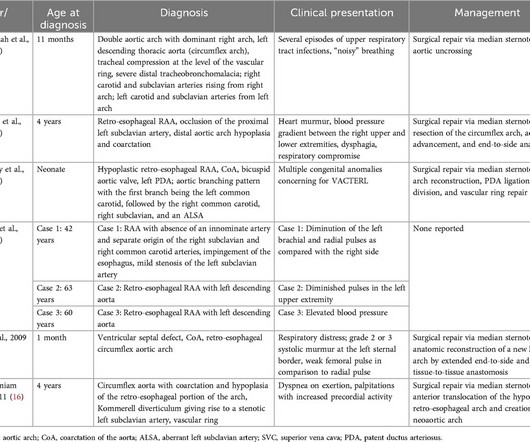
Circumflex right aortic arch is a rare aortic arch anomaly where the arch extends in a retro-esophageal pattern with a left-sided descending thoracic aorta. A 33-year-old G4P3 patient underwent fetal echocardiography after obstetric ultrasound showed concern for double aortic arch.
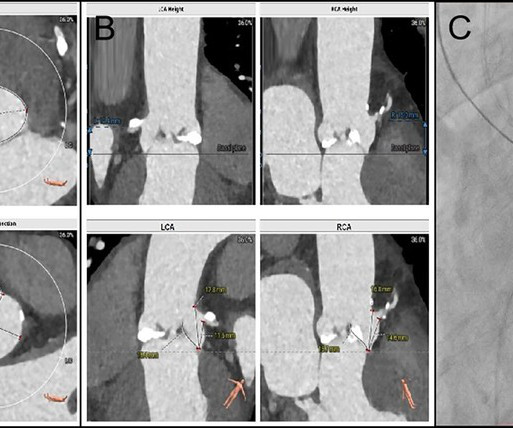
BackgroundFollowing transcatheter aortic valve replacement, acute coronary obstruction is infrequent but potentially life-threatening, while delayed coronary obstruction is even more uncommon.Case summaryA 69-year-old male underwent TAVR and subsequently developed an acute obstruction in the left main coronary artery.
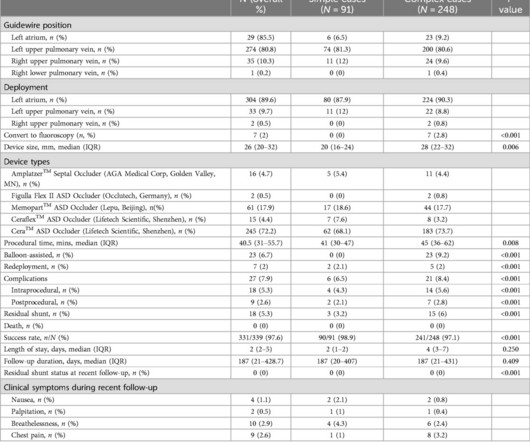
IntroductionZero-fluoroscopy, exclusively ultrasound-guided atrial septal defect (ASD) catheter closure has been reported. Complex cases included patients with large defects (25mm), multiple or fenestrated ASDs, deficient posterior-inferior rim <3mm, deficient retro-aortic rim <5mm, pulmonary hypertension, septal malalignment, and pregnancy.
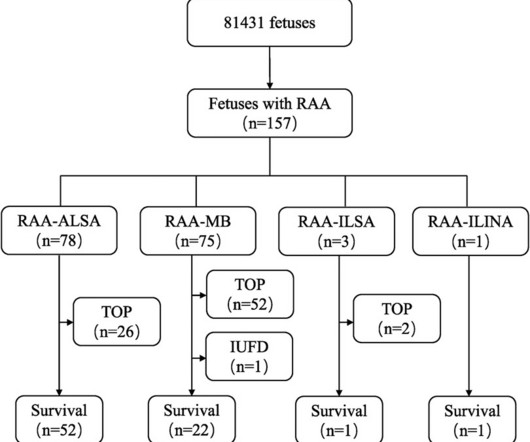
RAA features were characterised by comparing prenatal ultrasound data with anatomical casting results after pregnancy termination or postnatal imaging and surgical intervention to analyse the prognosis and misdiagnoses of fetal RAA.ResultsOf the 157 fetal RAA cases, 50 (31.8%) cases were isolated RAA and 107 (68.2%) cases were nonisolated RAA.
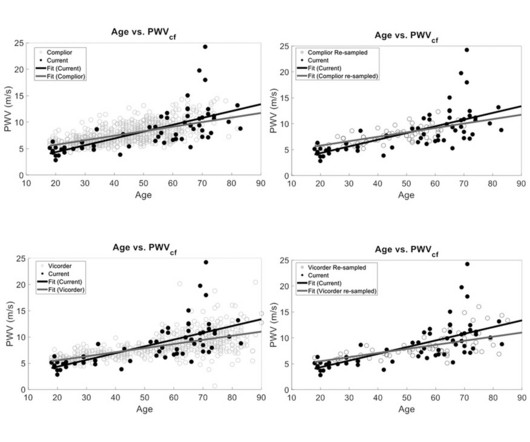
Ultrasound measured distensibility assessments confirmed the reliability of our PCG approach in reflecting central arterial stiffness dynamics, particularly at the aortic level. PWVcarotidtoe: 10.623.86 m/s) with age as a significant predictor (PWVcarotidfemoral: r2=0.45; PWVcarotidtoe: r2=0.28, p<0.05).
Fetal aortic valvuloplasty is considered for fetuses with severe valvar aortic stenosis and echocardiographic features suggesting a risk of progression to hypoplastic left heart syndrome. So if progression to hypoplastic left heart syndrome can be prevented by fetal aortic valvuloplasty, that would be theoretically a great boon.
During her doctoral research, Esther Maas investigated the use of new ultrasound techniques to image dangerous aortic aneurysms for patient-specific care.
Introduction Drug therapy to reduce the regurgitation fraction (RF) of high-grade aortic regurgitation (AR) by increasing heart rate (HR) is generally recommended. However, chronic HR reduction in HFREF patients can significantly improve aortic compliance and thereby potentially decrease RF. cm 2 hole in one aortic cusp.
Food and Drug Administration (FDA) has granted 510(k) clearance for its first-of-a-kind, AI-powered AISAP CARDIO point-of-care ultrasound (POCUS) software platform. We know that structural heart disease and heart failure are the leading causes of hospitalization and morbidity in the U.S.
Inverse probability weighting was used to assess the impact of IVUS on a composite outcome of repeat aortic intervention or death. Circulation: Cardiovascular Interventions, Ahead of Print.
Presentation title: QUALITY OF LIFE ASSESSMENT AT 30-DAYS FOLLOW-UP OF THE VALVOSOFT PIVOTAL STUDY ON SEVERE AORTIC VALVE STENOSE PATIENTS" (control number 16930) Time and date: April 8, 2024 - 9:32 a.m.–9:42 A summary of the poster session will be published on the Journal of the American College of Cardiology’s website.
milla1cf Thu, 05/02/2024 - 10:09 May 2, 2024 — Artificial intelligence experts at Cedars-Sinai and the Smidt Heart Institute created a dataset with more than 1 million echocardiograms, or cardiac ultrasound videos, and their corresponding clinical interpretations. Image by Getty.
Publication date: Available online 23 November 2024 Source: The American Journal of Cardiology Author(s): Taylor Pickering, Kyle McCullough, Cody Dorton, Emily Shih, Austin Kluis, Jasjit Banwait, Swapnil Gupta, Madhura Kapil Shah, Julius Ejiofor, William Brinkman, Justin Schaffer, J. Michael DiMaio, Katherine Harrington, Lee Hafen
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
Few of them currently have the equipment and expertise to diagnose valvular heart disease, but recent studies have demonstrated that healthcare professionals can use a combination of portable ultrasound devices and AI to diagnose heart diseases as well.
The blood culture revealed Rochebacterium caries, cardiac ultrasound detected vegetation, while brain and spleen abscesses manifested and progressively deteriorated. Despite a suboptimal response to anti-infective therapy, the patient ultimately underwent aortic valve replacement.
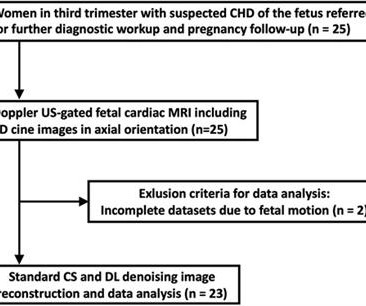
Purpose This study aims to evaluate deep learning (DL) denoising reconstructions for image quality improvement of Doppler ultrasound (DUS)-gated fetal cardiac MRI in congenital heart disease (CHD). Cine imaging was acquired using a balanced steady-state free precession (bSSFP) sequence with Doppler ultrasound gating. vs. 8.3 ± 3.6,
Publication date: Available online 18 May 2024 Source: The American Journal of Cardiology Author(s): Tomonari Shimoda, Mario D'Oria, Toshiki Kuno, Patrick Heindel, Sandro Lepidi, Mohamad A. Hussain, Hisato Takagi, Eric A.
Last week’s LumiGuide launch represents a step towards more widespread use, starting with major US and European Aortic Centers of Excellence for complex aortic repairs. Philips would then use the data it collects from this initial US and EU Aortic Center rollout to support a wider global launch.
510(k) clearance secured from FDA allows for EIQ’s AI-enabled solution, EchoSolv AS, to be marketed and sold in the USA Clearance marks a major milestone and will allow for rapid commercial scale-up EIQ is in advanced discussions with a range of US healthcare providers around the potential uptake of EchoSolv AS Working alongside US consultancy to obtain (..)
Additionally, we had to go to a high risk OBGYN for an additional ultrasound to make sure Austin’s heart chambers developed properly (everything appeared OK at the time). He was diagnosed with a butterfly vertebrae, kidney fullness, sacral dimple, and several heart defects (right aortic arch, VSD, and ASD).
The Queen of Hearts disagrees, diagnosing OMI with high confidence: Case Continued: The EKG was not immediately recognized by the emergency provider, who ordered a CT scan to rule out aortic dissection at 1419. If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia.
Meanwhile, over the years, ultrasound moved up from the pelvis, abdomen, right into coronary arteries and heart. Intravascular ultrasound-based interventions are being done in coronary artery, in a few cases to avoid contrast in patients with CKD. (We With zero radiation, MRI came close in the fight with innocuous proton imaging.
It was notable for a normal cardiac ultrasound with no pericardial fluid, normal LV and RV function (though the quality was not sufficient to evaluate for wall motion abnormalities) and normal IVC dynamics. A dissection flap is noted in the intrabdominal aorta, and the aortic outflow tract is also noted to appear wider than normal.
Description of Case:A 64-year-old male with complex medical history, including infective endocarditis of the aortic valve requiring surgical replacement with a bioprosthetic valve and recurrent infective endocarditis of the bioprosthetic valve, presented with two hours of crushing chest pain and found to have ST elevations.
Focusing on mitral and tricuspid valve diseases , Capstans treatment combines transcatheter implantation of a folded valve replacement with its X-ray and ultrasound-guided robot to align the low-profile implant with the beating heart valve.
Smith comment: This patient did not have a bedside ultrasound. Had one been done, it would have shown a feature that is apparent on this ultrasound (however, this patient's LV function would not be as good as in this clip): This is recorded with the LV on the right. Look at the aortic outflow tract. What do you see?
We describe a fetus with prenatal echocardiographic findings of BDA and right aortic arch mirror-image branching (RAA-MIB) combined with congenital heart disease. Prenatal ultrasound diagnosis of BDA is important and requires a combination of 2D grayscale, CDFI, and STIC images to assist in scanning.
We aimed ultrasound-guided punctures in the proximal two-thirds of axillary arteries with diameters ≥2 mm to insert 7 cm/4 Fr short introducers. Overall, 27/36 procedures were interventional, including 6 aortic valvuloplasties, 6 balloon angioplasties, and 15 stenting procedures. We administrated intra-arterial verapamil (1.25 mg)
Serial echocardiographic assessments are common in clinical cardiology, e.g., for timing of intervention in mitral and aortic regurgitation. When following patients with serial echocardiograms, each new measur.
What is the evidence for intra-aortic balloon pumps, percutaneous ventricular assist devices and ECMO in the patient with cardiogenic shock? What are the best strategies to efficiently get the patient in cardiogenic shock to definitive care, whether that be the cath lab or the operating room?
Although indexing effective orifice area (EOA) by body surface area (BSA) is recommended, this method has several disadvantages, since it corrects by acquired fatty tissue. Our aim was to analyze the value of.
The next morning the patient went for his routine echocardiogram, where the operator noticed a dilated aortic root at 5.47 cm with severe aortic insufficiency. The team was notified and they ordered a stat aortagram which showed type A aortic dissection from the aortic valve to the iliacs. Pericarditis?
The procedure was initiated via ultrasound‐guided right common femoral access. When opting for such an approach it is vital to factor in the aortic arch appearance and its branches. ASPECT score 5‐6. The patient was deemed a candidate for mechanical endovascular thrombectomy (MER).
Blunt cardiac injury my result in : 1) Acute myocardial rupture with tamponade 2) Valve rupture (tricuspid, aortic, mitral) 3) Coronary thrombosis or dissection (and thus Acute MI) from direct coronary blunt injury 4) Dysrhythmias of all kinds. In the ED, ultrasound showed hemopericardium with tamponade.
An intra-aortic balloon pump was placed, and the patient was taken for immediate surgical repair but did not survive. If detected early by ultrasound, the patient can be saved. An echocardiogram showed no hemopericardium, but D oppler showed a new small ventricular septal defect with left to right shunting. 3) Oliva et al. (4)
During medical school, one of the classic bedside exam questions we get is how to differentiate the valve issues of aortic stenosis and mitral regurgitation, which produce similar but different murmurs when you listen with a stethoscope. “How can you tell the difference between aortic stenosis and mitral regurgitation at the bedside?”
During echocardiography, a transducer transmits the ultrasound beam towards the heart. Opening and closing movements of the aortic and mitral valves are visible. The image shows the blue coloured descending aortic flow on colour Doppler. Hence a basic knowledge is needed for all physicians and paramedics.
2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. Widespread ST-depression with reciprocal aVR ST-elevation can be cause by: Heart rate related: tachyarrhythmia (e.g., Initial blood work showed the following: metabolic acidosis on VBG with a lactate of 7.1; Left main? 3-vessel disease?
Due to the severity of the pain and the high BP, they obtained an aortic dissection CT. Regional wall motion abnormality-inferolateral (this is the formal ultrasound location of a posterior wall motion abnormality). especially since this Chest CT was done to rule out aortic dissection ). Here is a case from a while back.
An elderly patient with a ruptured abdominal aortic aneurysm: Formal ECG Interpretation (final read in the chart!) : "Inferior ST elevation, lead III, with reciprocal ST depression in aVL." A bedside ultrasound was done by the emergency physician, using Speckle Tracking. What do you think? Unfortunately, that video is unavailable.
Rob Simard discusses one of the most important uses of POCUS in the ED, and that is for AAA. He reviews the literature on the accuracy of POCUS for AAA as well as demonstrates the limitations and the common pitfalls in this POCUS Cases video.
CT angiogram chest: no aortic dissection or pulmonary embolism. Beware a negative Bedside ultrasound. He spent several days in the PICU, undergoing workup including: Serial troponins: rising from 5,700 ng/L (unknown if I or T) to greater than 25,000 ng/L (greater than the lab's upper limit of reporting). Pericarditis?
Venn diagram highlighting the main similarities and differences between heart failure with preserved ejection fraction (HFpEF) and aortic stenosis with preserved ejection fraction (ASpEF). Patients with ASpEF eligible for transcatheter aortic valve replacement ( n = 125) also performed cardiac computed tomography (CT).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content