This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
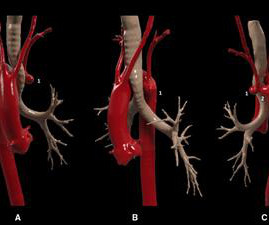
In this case, we present a symptomatic patient with a Kommerell's diverticulum and a left aberrant subclavian artery complicated by proximal stenosis and poststenotic aneurysm.
Some of the late-breaking topics that will be covered include transcatheter aortic valve replacement (TAVR), peripheral artery disease (PAD), and pulmonary embolism (PE): Impact of Age on Procedural Timing for Asymptomatic Severe AorticStenosis: Results from the Early TAVR Trial The PERFORMANCE II Trial: A Prospective Multicenter Single Arm Investigation (..)
Transcatheter aortic valve replacement (TAVR) is the standard treatment for severe aorticstenosis, but post-TAVR leaflet thrombus, identified by hypoattenuated leaflet thickening (HALT), poses potential risks like cerebral thromboembolic events. had thrombus at any aortic valve complex. Specifically, 14.2%
This next-generation surgical aortic tissue valve is designed to facilitate ease of use at implant and lifetime patient management. It’s an excellent choice for cardiac surgeons and their patients seeking an aortic valve solution that can be fit for the future, right from the start. 5 Verbelen T, Roussel JC, Cathenis K, et al.,
This next-generation surgical aortic tissue valve is designed to facilitate ease of use at implant and lifetime patient management. It’s an excellent choice for cardiac surgeons and their patients seeking an aortic valve solution that can be fit for the future, right from the start. 5 Verbelen T, Roussel JC, Cathenis K, et al.,
Stenosis of the external carotid artery in such patients can be a source of atheroembolism or hypoperfusion. We describe a case of external carotid stenting with carotid stump coil occlusion.MethodsWe present a case report.
Coronary angiography gives a visual impression about the severity of the stenosis. But it need not imply the actual functional significance of the stenosis in terms of flow physiology. If the FFR normalizes after stenting, the restenosis rates at six months is less than 5%. Normal FFR is 1.0 and an FFR below 0.75 in the study.
The phantom includes the aortic arch, all supraoptic cervical arteries and a complete circle of Willis up to the M2‐MCA, A2‐ACA and P2‐PCA segments. 3% sodium alginate solution was cast into a stenosis mold and crosslinked in a 40% calcium chloride. An initial stenosis flow rate was registered with a value of 8.5 ± 5.33
The Queen of Hearts disagrees, diagnosing OMI with high confidence: Case Continued: The EKG was not immediately recognized by the emergency provider, who ordered a CT scan to rule out aortic dissection at 1419. This was a presumed culprit and a stent was placed. The ST depressions in I and aVL have resolved.
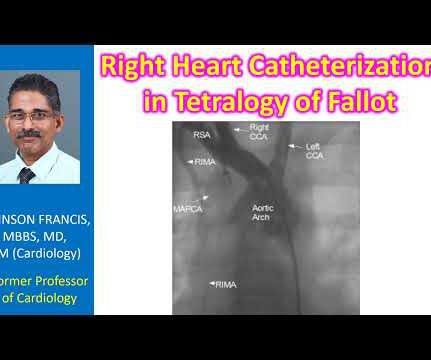
Findings which are sought during an aortogram in tetralogy of Fallot include looking for aortic regurgitation, coronary anomalies, MAPCAs, patent ductus arteriosus and side of the aortic arch. Stenting of the patent ductus arteriosus can be considered in neonatal period for improving oxygen saturation till corrective surgery.
However, CTA head and neck 4 days later demonstrated 90 percent stenosis of the mid left V2 at the C3‐4 level and a 75‐90 percent stenosis of the left mid V2 segment at the C5‐6 level (hard and soft plaque in these areas). He also had moderate stenosis of the right V4 segment.
SMART 4 ( NCT04722250 ) studied patients with severe aorticstenosis and a small aortic annulus who underwent transcatheter aortic valve replacement (TAVR). The primary non-inferiority endpoint was MACCE (a composite of cardiac death, MI, ischaemic stroke, stent thrombosis, or target vessel revascularisation).
The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aorticstenosis. We also looked at his aortic root by both parasternal and suprasternal views, and the aorta was normal.] I called the cardiologist on call and we agreed that we needed to activated the cath lab.
60-something with h/o MI and stents presented with chest pain radiating to the back and nausea/vomiting. There was concern for aortic dissection, so a CT was done and was negative. It was stented. The patient had a p rior h istory of MI + stents. Time zero What do you think? There is inferior ST elevation. Pericarditis?
LAD plaque with 0-25 percent stenosis. No signs for aortic dissection or pulmonary embolus. --"Results were discussed with the ordering physician. The LAD has moderate 40% ostial-proximal LAD stenosis and severe 90% mid LAD stenosis involving first diagonal branch. --The A CT Coronary angiogram was ordered.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. An elderly patient with a ruptured abdominal aortic aneurysm: Formal ECG Interpretation (final read in the chart!) : "Inferior ST elevation, lead III, with reciprocal ST depression in aVL." This is a very common misread. What do you think?
There is ventricular hypertrophy in the absence of abnormal loading conditions, such as aorticstenosis, or hypertension, for example – of which the most common variant is Asymmetric Septal Hypertrophy. A mid-LAD culprit lesion was identified and stented.
61,62) The interventional community defines occlusive LM disease as >50% by FFR, or ≥75% stenosis,(63) but urgent or emergent intervention on lesions not meeting these thresholds is only imperative if it is a thrombotic lesion and the patient has refractory ischemic symptoms (i.e. TIMI 0/1 flow).(61,62) Knotts et al.
Adult Cardiac Surgery Database Lead Author Title Publication Date Jacob Raphael Red Blood Cell Transfusion and Pulmonary Complications: The Society of Thoracic Surgeons Adult Cardiac Surgery Database Analysis The Annals of Thoracic Surgery January 2024 Joseph Sabik Multi-Arterial versus Single-Arterial Coronary Surgery: Ten Year Follow-up of One Million (..)
Program Designations Access and Publications (A&P) 1 Participant User File (PUF) 2 Task Force on Funded Research (TFR) 3 Special Projects 4 Adult Cardiac Surgery Database Lead Author Title Publication Date William Keeling 2 National Trends in Emergency Coronary Artery Bypass Grafting European Journal of Cardiothoracic Surgery October 2023 Jake (..)
No thoracic aortic hematoma, aneurysm or dissection. First obtuse marginal also had an 80% stenosis and was stented. Patient states pain improved on ambulance ride over after receiving 325 mg Aspirin and nitroglycerin, with pain down to 2/10. CT Angio Chest IMPRESSION 1. No pulmonary embolism is identified.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content