This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Due to the chest pain radiating into the patient's back, the ER physician ordered CTA chest to rule out aortic dissection. The cardiologist agreed that the ECG was suggestive of STEMI, but the facility's cath lab was apparently not available and he therefore recommended emergent transfer to a cath capable facility.
Microvascular resistance evaluated whether the vasodilatory reserve capacity of coronary microcirculation was restored in the infarcted territory, regardless of concomitant epicardial coronary artery disease and aortic pressure. Immediate Microvascular Physiology After Mechanical Coronary Reperfusion of STEMI. J Am Coll Cardiol.
Leriche syndrome (1948, Annals of Surgery, College de Paris, France) is a famous eponym in Aortic vascular emergency, where a saddle-shaped thrombus folds across the Aortic bi-furcation resulting in bilateral lower limb vascular insufficiency. The Syndrome of Thrombotic Obliteration of the Aortic Bifurcation. Reference 1.Leriche
In this ECG Cases blog we look at 10 cases of patients with chest pain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
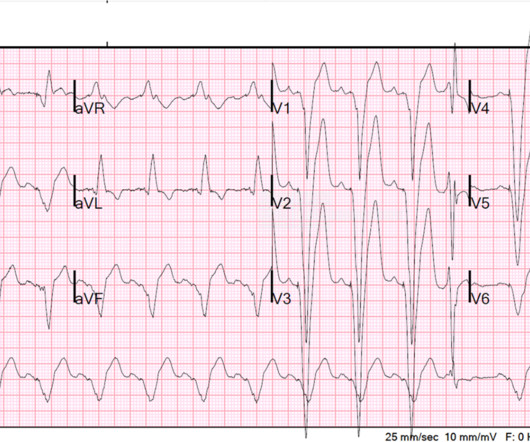
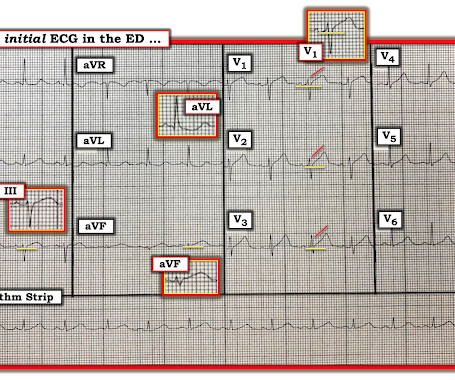
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. the presence of such well developed, wide, anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
As his pain was very severe, emergency physicians concerned of aortic dissection and ordered a thoracic CT scan. Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. --In summary, some subtle findings which do not fit into a pattern, therefore may be nonspecific ECG changes which are encountered everyday.
Which patients with ECG evidence of coronary occlusion require a CT scan to rule out aortic dissection? What are the range of ECG findings in acute aortic dissection and how do they change management? Dr. Jesse McLaren guides us through 9 cases to answer these and other questions on ECG interpretation in aortic dissection.
The Queen of Hearts disagrees, diagnosing OMI with high confidence: Case Continued: The EKG was not immediately recognized by the emergency provider, who ordered a CT scan to rule out aortic dissection at 1419. Most STEMI have peak troponin I over 1000 ng/L and most NSTEMI below that level.
Left ventricular afterload reduction is essential to decrease the trans-se ptal pressure gradient and thus decrease shunt volume, making a larger proportion of the blood flow from the left ventricle through the aortic valve. A mong patients with STEMI, ventricular septal rupture is the most common and free wall rupture is the least common.
is very specific for STEMI , and there is some evidence, as well as rationale, that a paced rhythm behaves similarly. Here is one case of anterior STEMI in a paced rhythm. Here is a case of lateral STEMI in a paced rhythm. He has had previous angiograms showing "large vessels" and "no significant coronary disease."
An echocardiogram confirmed aortic stenosis with a large pressure gradient. Thus, this patient had increased ST elevation (current of injury) superimposed on the ST elevation of LVH and simulating STEMI. The next day, and angiogram showed normal coronary arteries. He awoke and did well.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
The provider contacted cardiology to discuss the case, but cardiology "didn't think it was a STEMI, didn't think he needed emergent cath." JAMA 2000) showed that 1/3 of patients with STEMI, and 1/3 of patients with NSTEMI, present without chest pain. The whole paradigm is literally called "STEMI" vs. "NSTEMI." Canto et al.
QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. Two weeks ago he had a significant MVC with many severe injuries, including aortic injury s/p endovascular repair. I sent this to our group without information and Dr. Smith responded: "Not OMI.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? J Electrocardiol 2013;46:240-8 2. Left main?
The "criteria" for posterior STEMI are 0.5 Is it STEMI or NonSTEMI? The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. We also looked at his aortic root by both parasternal and suprasternal views, and the aorta was normal.]
The estimated left ventricular ejection fraction is 58 % Aortic stenosis, mild, 9.0 We found that 38% of out of hospital ventricular fibrillation was due to STEMI. Correlation of STEMI in Resuscitated Non-traumatic out-of-hospital Cardiopulmonary Arrest patients with Initial Rhythm and Cardiac Catheterization Findings (Abstract 580).
Look at the aortic outflow tract. Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve.
Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. They also wanted an aortic CT which was negative. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Is it normal STE? However , there is terminal QRS distortion in lead V3.
It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. An elderly patient with a ruptured abdominal aortic aneurysm: Formal ECG Interpretation (final read in the chart!) : "Inferior ST elevation, lead III, with reciprocal ST depression in aVL."
Patients with documented STEMI, left ventricular thrombus, mechanical mitral or aortic valve replacement were excluded. ICD 10 codes were used to identify patients with documented a fib. Procedure ICD codes were used to identify patients that underwent percutaneous LAAO. 5,661 underwent percutaneous closure. years with STD 7.86.
But limitation of this ST elevation to a single lead is not consistent with any distribution of a STEMI. The plan was to proceed as soon as possible with aortic valve replacement. This patient needed prompt aortic valve replacement. Then there is the significant ST elevation we see in lead V1.
The next morning the patient went for his routine echocardiogram, where the operator noticed a dilated aortic root at 5.47 cm with severe aortic insufficiency. The team was notified and they ordered a stat aortagram which showed type A aortic dissection from the aortic valve to the iliacs. Pericarditis?
This has important clinical significance , as many successfully lysed STEMI patient might have minimal segments of dissection/deep plaque fissures. , Mind you, even if it occurs, it is atypical, continuous, non-anginal if flow is unaffected, and not relieved by nitro-glycerine. may be misdiagnosed as post infarct angina.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
The patient arrived looking like an aortic dissection patient, so CTA was done and negative." OMI often does not meet STEMI criteria. If you rely on STEMI criteria, or on the computer algorithm, many of your patients will progress to a completed MI. ST elevation at 60 ms after the J-point in lead V3 = 1.5
Due to the severity of the pain and the high BP, they obtained an aortic dissection CT. Here is the repeat ECG at 52 minutes after arrival to triage: Obvious posterolateral STEMI Angiographic findings: 1. Comparison of the ST-Elevation Myocardial Infarction (STEMI) vs. NSTEMI and Occlusion MI (OMI) vs. NOMI Paradigms of Acute MI.
A repeat ECG was done: Obvious anterolateral wall STEMI. On arrival his BP was 70s/40s, so an intra-aortic ballon pump was placed. This rhythm reportedly produced no palpable pulse, and CPR was continued. 30 seconds later, however, the patient began spontaneously moving and CPR was discontinued.
There is ventricular hypertrophy in the absence of abnormal loading conditions, such as aortic stenosis, or hypertension, for example – of which the most common variant is Asymmetric Septal Hypertrophy. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital.
No signs for aortic dissection or pulmonary embolus. --"Results were discussed with the ordering physician. Thus, Wellens' syndrome should be thought of as a transient OMI or transient STEMI. Transient STEMI is at high risk of re-occlusion. A CT Coronary angiogram was ordered. LAD plaque with 0-25 percent stenosis.
50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. CT angiogram chest: no aortic dissection or pulmonary embolism. 24 yo woman with chest pain: Is this STEMI?
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. An EKG from a year prior was available for comparison: The ED physician noted Initial EKG here read by the computer as a STEMI, however, there is a very poor baseline and a lot of artifact. See reference and discussion below.
His first EKG is shown below, with a lead II rhythm strip: EKG 1, 1645 A provisder who is looking for STEMI would not see much in this EKG. It is possible that the T waves in this EKG are of an intermediate morphology between full-blown STEMI and inferior reperfusion. This is the classic morphology of hyperacute T waves.
That said — the overall picture to me did not "look" acute — and the history of "chest pain radiating to the back " in this 80-something man with marked LVH — made me strongly consider an aortic dissection as a more likely cause. And, even if there was acute aortic dissection — the dissection could result in occlusion of a coronary artery.
His initial high sensitivity troponin I returned at 1300 ng/L and given that his cardiac workup was otherwise unremarkable, a CT was obtained to evaluate for pulmonary embolism and aortic aneurysm or dissection but this too was unrevealing. Another EKG was also obtained. ECG at time 82 minutes: What do you think?
50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). Larger shunt volume means less blood exiting the left ventricle through the aortic valve and lower cardiac output. See Raitt et al.:
It is diagnostic of OMI, but this is SUBACUTE OMI I sent this ECG to my "EKG Nerdz" friends, without any clinical info at all and they answered "OMI" The Queen said: "STEMI-Equivalent with High Confidence:" Notice she sees findings in both normal beats and PVCs. If this were ACUTE (vs.
The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". No thoracic aortic hematoma, aneurysm or dissection. Pt received 324 ASA and 2 sprays of nitro with improvement. Cath lab was activated by EMS and transported emergent." Pain was decreased to 2/10. CT Angio Chest IMPRESSION 1.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content