This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BackgroundProtruding aorticplaque is known to be associated with an increased risk for future cardiac and cerebrovascular events. Coronary plaque characteristics were compared to evaluate coronary plaque vulnerability in patients with protruding aorticplaque on computed tomography angiography.
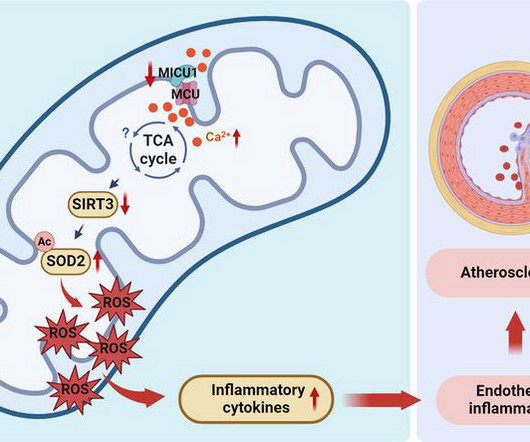
Of clinical relevance, we observed decreased MICU1 expression in the endothelial layer covering human atherosclerotic plaques and in human aortic endothelial cells exposed to serum from patients with coronary artery diseases (CAD).
BackgroundComplex aorticplaque (CAP) is a potential embolic source in patients with cryptogenic stroke (CS). Most studies (74%) used ≥4 mm plaque thickness as the imaging criterion for CAP although ≥1 mm (N=1, CTA), ≥5 mm (N=5, TEE), and ≥6 mm (N=2, CTA) were also reported. 0.41],I2=94%). I2=95%) for TEE; 0.23 (95% CI, 0.15–0.34;I2=87%)
Lp(a) is emerging as an important, yet under-recognized, potential risk factor for cardiovascular disease due to its ability to promote the development of plaques within artery walls, clot formation and aortic valve calcification. 2022 Aug, 80 (9) 934946 Kronenberg F.
Background:The bovine aortic arch is a vascular variant in which the left common carotid artery originates from the brachiocephalic trunk rather than directly from the aortic arch. The bovine anatomical variation may alter the blood flow dynamics, potentially contributing to the formation and progression of carotid plaques.
Sections of coronary atherosclerotic plaques from donors were immunostained to analyze calcium deposition and 4-HNE. 4-HNE promoted calcification of both mouse aortic smooth muscle cells and human aortic smooth muscle cells and their osteochondrogenic differentiation in vitro.
The Queen of Hearts disagrees, diagnosing OMI with high confidence: Case Continued: The EKG was not immediately recognized by the emergency provider, who ordered a CT scan to rule out aortic dissection at 1419. Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing?
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
Irradiation of 282 nm UV‐B but not 301 or 312 nm UV‐B significantly reduced the development of aortic root atherosclerotic plaques and plaque inflammation.
This has important clinical significance , as many successfully lysed STEMI patient might have minimal segments of dissection/deep plaque fissures. , Kim N Engl J Med 2020; 383:2358-2370 Next query What is the difference between plaque fissure and coronary arterial dissection? Is plaque fissure painful ?
Mice lackingFxrandGpbar1−/−/Fxr−/−display hypotension and aortic inflammation, along with altered intestinal permeability that deteriorates with age, and severe dysbiosis, along with dysregulated bile acid synthesis. Vasomotor activities of aortic rings were altered byGpbar1andFxrgene ablation.
Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates). The underlying etiology is either Type 1 or Type II ischemia, although sometimes there’s overlap of both. Type I ischemia. Type II ischemia.
Description of Case:A 64-year-old male with complex medical history, including infective endocarditis of the aortic valve requiring surgical replacement with a bioprosthetic valve and recurrent infective endocarditis of the bioprosthetic valve, presented with two hours of crushing chest pain and found to have ST elevations.
With its advantage of shape and stiffness buffering the kickback force with support of lesser curvature of aortic arch, BGCs were navigated to the appropriate position without touching to the plaques.ResultsThe technique were applied in 5 cases (age: 73‐85 years old, 4 males, 4 left‐sided lesions) among the 37 consequent CAS cases.
A 69‐year‐old woman with a history of lung cancer, hypertension, chronic tobacco use, atherosclerosis, and known calcified plaque at the left carotid bifurcation on dual antiplatelet therapy presented with acute onset of expressive aphasia and right hemiparesis due to acute left CCAO.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. elevated BP), but rather directly correlated with coronary obstruction (due to plaque rupture and thrombosis) and, potentially, stymied TIMI flow. Aortic Stenosis f.
The phantom includes the aortic arch, all supraoptic cervical arteries and a complete circle of Willis up to the M2‐MCA, A2‐ACA and P2‐PCA segments. The phantom includes the aortic arch, all supraoptic cervical arteries and a complete circle of Willis up to the M2‐MCA, A2‐ACA and P2‐PCA segments.
However, CTA head and neck 4 days later demonstrated 90 percent stenosis of the mid left V2 at the C3‐4 level and a 75‐90 percent stenosis of the left mid V2 segment at the C5‐6 level (hard and soft plaque in these areas). He was switched from DAPT to aspirin and warfarin because he was considered a “DAPT failure.”
2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. Widespread ST-depression with reciprocal aVR ST-elevation can be cause by: Heart rate related: tachyarrhythmia (e.g., Initial blood work showed the following: metabolic acidosis on VBG with a lactate of 7.1; Left main? 3-vessel disease?
LAD plaque with 0-25 percent stenosis. No signs for aortic dissection or pulmonary embolus. --"Results were discussed with the ordering physician. Now, with elevated troponins, Wellens' syndrome is likely. A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD
BACKGROUND:Aortic arch plaques are associated with an increased risk of ischemic stroke in patients with cryptogenic stroke or prior embolic events. Arch plaques were assessed by suprasternal transthoracic echocardiography; plaques ≥4 mm in thickness were classified as large plaques. Stroke, Ahead of Print.
There are multiple possible clinical situations that could account for diffuse subendocardial ischemia that is not due to ACS and plaque rupture. Post PCI an intra-aortic balloon pump (IABP) was placed and a combination of norepinephrine and dobutamine was needed to maintain perfusion pressures.
Mechanistically, HEG1 knockdown prevented s-flow–induced KLF2/4 (Krüppel-like factor 2/4) expression by regulating its intracellular binding partner KRIT1 (Krev interaction trapped protein 1) and the MEKK3-MEK5-ERK5-MEF2 pathway in human aortic endothelial cells.
SMART 4 ( NCT04722250 ) studied patients with severe aortic stenosis and a small aortic annulus who underwent transcatheter aortic valve replacement (TAVR). The study concluded that among low-risk patients with severe aortic stenosis, TAVI is as effective as SAVR in terms of the composite outcome of death or stroke at 1 year.
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 1,2 ASCVD causes or contributes to conditions that include coronary artery disease (CAD), cerebrovascular disease, and peripheral vascular disease (inclusive of aortic aneurysm).3
CT angiogram chest: no aortic dissection or pulmonary embolism. Only after her troponin peaked at 500,000 ng/L did she get her angiogram, which showed a 100% left main occlusion due to ruptured plaque. No further troponins were measured. Serial chest xrays: progressive bilateral pulmonary edema. Diagnostic of Massive OMI.
This was ruptured plaque with thrombus. Important: It is exceedingly rare for an anterior STEMI to be due to Aortic Dissection. Here it is: Type A Aortic Dissection Why was the troponin so elevated? of STEMI are due to Aortic Dissection. And almost all of them could be detected by bedside ultrasound. This is easy to see.
High Lp(a) is a causal risk factor for atherosclerotic cardiovascular disease (ASCVD), aortic stenosis, and all-cause mortality. Elevated Lp(a) is associated with complex, difficult-to-treat atherosclerotic lesions and fast-progressing plaques.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content