This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A significant proportion of patients with severe aortic stenosis (AS) undergoing transcatheter aortic valve implantation (TAVI) have concomitant coronary artery disease (CAD). A better understanding of how we assess and interpret coronary physiology in these patients is required to optimise treatment pathways.
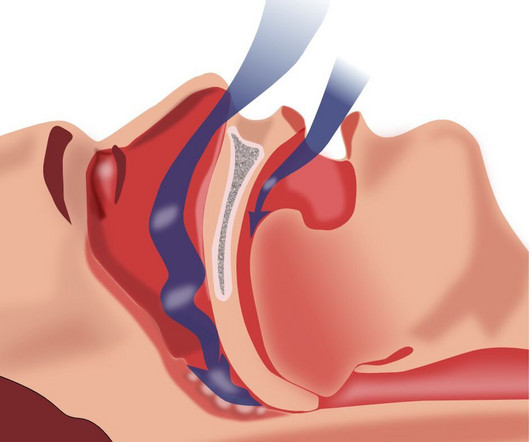
Obstructive sleep apnea may be a risk factor for developing abdominal aortic aneurysms, according to researchers from the University of Missouri School of Medicine and NextGen Precision Health.
MC1R recessive yellow mice showed blunted hypertrophic response to transverse aortic constrictioninduced pressure overload and exercise training. Mice were phenotyped for cardiac structure and function by echocardiography, histology, and quantitative PCR analysis.
Ruptured abdominal aortic aneurysms (rAAA) remain one of the most clinically challenging and technically complex emergencies in contemporary vascular surgery practice. Moreover, evolution in pre- and post-operative physiologic resuscitation has also contributed to observed improvements in rAAA outcomes.
Digging into and unravelling the pathogenesis of AD will aid in exploring novel therapeutics for AD.The major characteristics of AD is degeneration of aortic wall architecture. Different segments of mouse aorta were subjected to EVG staining to examine the aortic wall architecture.Real-time quantitative PCR (qPCR).
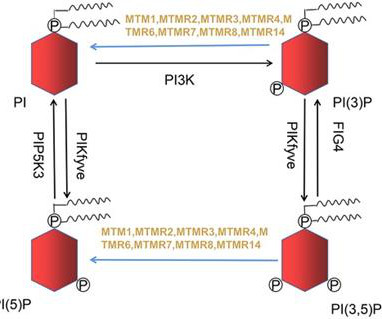
Based on the ability of modulating the levels of these PIPs, MTMRs exert physiological functions such as vesicle trafficking, cell proliferation, differentiation, necrosis, cytoskeleton, and cell migration. This review summarizes the functions of MTMRs and highlights their pathophysiological roles in cardiovascular diseases.
No doubt ,the Aortic interventional world is applauding and everyone is joining the party. Apart from valve size aortic annular enlargement before SAVR was not done in majority, there by enhancing the gradient and valve mis-match.(Note Flow is physiology. Now, some academic queries ? Because it was done in 2010-2013.
The pump is delivered into the heart fully sheathed, over a guidewire, through the aorta, and across the aortic valve. It further notes the following on the technology: The Elevate pump is first folded and then inserted percutaneously through a small puncture in the groin to accommodate a commercially available 10 Fr introducer sheath.
Microvascular resistance evaluated whether the vasodilatory reserve capacity of coronary microcirculation was restored in the infarcted territory, regardless of concomitant epicardial coronary artery disease and aortic pressure. Immediate Microvascular Physiology After Mechanical Coronary Reperfusion of STEMI. J Am Coll Cardiol.
Two weeks ago he had a significant MVC with many severe injuries, including aortic injury s/p endovascular repair. Serial echo monitoring showed increasing pericardial pressures without overt tamponade physiology. CT angiogram showed stable TEVAR without complications. ESR and CRP were both highly elevated.
An Aortic Impella device, that is distal to the aortic valve and devoid of LV-related issues. The hemodynamic of the Giraffe’s vascular system is a good physiologic model of circulation, that defy gravity. Shall we think about,axial pumps in ascending Aorta in series with LV.
The integrative physiology of the left ventricle and systemic circulation is fundamental to our understanding of advanced heart failure and cardiogenic shock. In simplest terms, any increase in aortic stiffness increases the vascular afterload presented to the failing left ventricle. Circulation: Heart Failure, Ahead of Print.
Look at the aortic outflow tract. The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Aortic angiogram did not reveal aortic dissection. In fact, bedside ultrasound might even find severe aortic stenosis. What do you see?
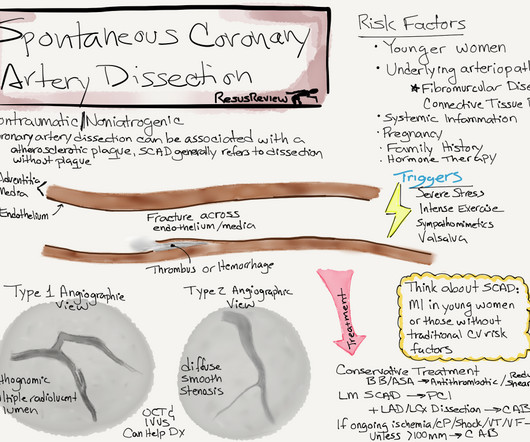
Spontaneous coronary dissection vs Iatrogenic dissection SCAD is a rare , different entity , enjoys a popular space in the patho-physiology of CAD. This has important clinical significance , as many successfully lysed STEMI patient might have minimal segments of dissection/deep plaque fissures. , may be misdiagnosed as post infarct angina.
While each device has a different physiological impact on the heart, limited studies compare genetic changes in the heart t-MCS. Background:Various temporary mechanical circulatory support device (t-MCS) options are available for supporting patients in cardiogenic shock. and 4 bridged with IABP.
The phantom includes the aortic arch, all supraoptic cervical arteries and a complete circle of Willis up to the M2‐MCA, A2‐ACA and P2‐PCA segments. mL/min.ConclusionThe developed ICAD model is anatomically accurate and offers realistic physiological and procedural features.
Dr. Folesani, who is accomplished in performing aortic and mitral valve surgery and myocardial revascularization procedures, intends to use his fellowship to learn minimally invasive techniques on aortic and mitral valves. “I For more information, visit eacts.org.
There could be enlargement of aorta, neoaorta, producing annuloaortic ectasia and aortic regurgitation, another long term sequelae of arterial switch operation. This is diagrammatic representation of another of the complications, delayed sequelae of arterial switch. Long term results are much better than atrial switch operations.
The first troponin returned at 0.099 ng/mL (elevated, consistent with Non-Occlusion MI) Providers were concerned with aortic dissection, so they order a chest aorta CT. It just doesn’t make good physiologic sense for there to be an rSr’ only in lead V2, and not in V1. It is essentially normal.
Getty Images milla1cf Fri, 06/07/2024 - 15:10 June 7, 2024 — Calcific aortic valve disease (CAVD) is the major heart valve disease that afflicts nearly 10 million patients globally with an annual mortality exceeding 100,000, and the numbers continue to rise. These findings appear online in the journal Trends in Molecular Medicine.
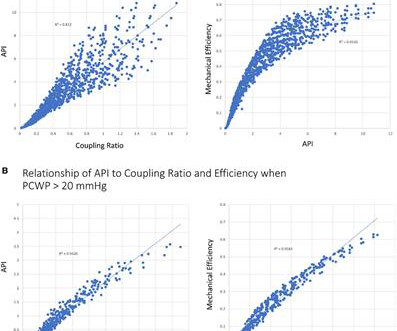
Methods Here, a mathematical and physiological framework to define the patient-specific tipping point of myocardial energetics is defined. A novel hemodynamic parameter known as the myocardial performance score (MPS), a marker of power and efficiency, is introduced that allows for the objective assessment of the physiological tipping point.
Written by Pendell Meyers A woman in her 20s with connective tissue disorder and history of aortic root and valve repair presented with palpitations. Further history revealed she had new onset atrial flutter soon after her aortic surgery, and was put on flecainide approximately 1 month ago. Here is her triage ECG: What do you think?
But it need not imply the actual functional significance of the stenosis in terms of flow physiology. FFR is obtained by dividing the pressure distal to the stenosis by the central aortic pressure, which is usually equal to the pressure proximal to the stenosis if there is no additional stenosis in between. Normal FFR is 1.0
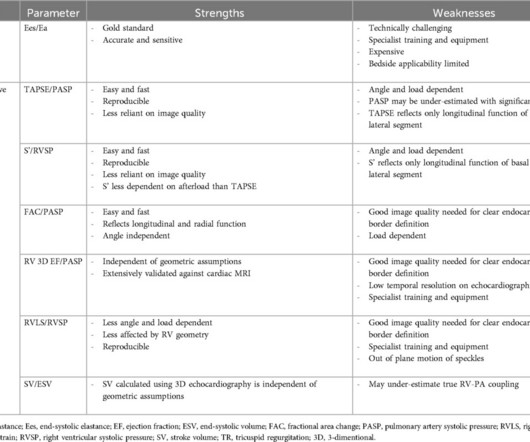
Aortic stenosis (AS) was historically considered a disease of the left side of the heart, with the main pathophysiological impact being predominantly on the left ventricle (LV). This review will summarise the features of normal RV physiology and the mechanisms responsible for RV impairment in AS.
13 Coronary artery calcification (CAC) and aortic stiffness are also associated with self-reported sleep duration. 21 22 23 It is worth noting that the literature here is still in its infancy, as research into sex differences is currently an emerging area in physiology.
Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. heart auscultation (aortic stenosis); c. Fourth, syncope in the elderly often results from polypharmacy and abnormal physiologic responses to daily events. Good History and Physical exam, including a. orthostatic vitals b. FHx of sudden death.
It needs a good knowledge of anatomy, physiology of inter & Intra valvular hemodynamics.It Final message Prosthetic valve assessment is complex, thought process intensive examination. Not every echocardiographer can do it efficiently.
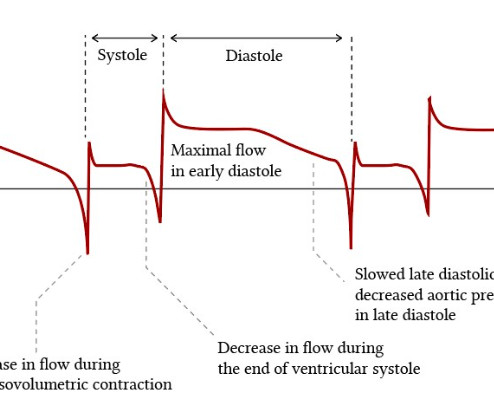
The classical illustrations that are found in cardiac physiology literature about the dominance of coronary blood flow during diastole (Image source Ref 2) Instead, coronary perfusion pressure, mean coronary arterial pressure, and coronary arterial wedge pressure are discussed. How common is angina in DCM ? Reference 1. Green, Donald D.
A bedside echo revealed the large pericardial effusion, with tamponade physiology confirmed clinically and ultrasonographically. CT done to look for aortic dissection. This is electrical alternans. Here is her initial ED ECG: Here is a prior ECG available from months ago: No alternans.
Innocent Heart Murmurs: These are also called functional or physiologic murmurs. The aortic valve and mitral valve are two of the most common valves affected by heart murmurs. Aortic stenosis, mitral valve prolapse, and other valve problems may not resolve without treatment. Innocent murmurs do not indicate a heart problem.
Hemodynanmic of normal delivery Natural delivery involves the physiological stress of labor, which includes increased cardiac output, blood pressure fluctuations, and oxygen demand, peaking at 50-80% above baseline during contractions and pushing. In women with significant heart disease, the physiological demands of labor (e.g.,
The QoH now correctly sees active OMI: A CT scan to rule out aortic dissection was performed (Smith: why???) The physiologic reason for this finding is that the T wave axis in the limb leads generally follows the QRS axis. Hans has not even been to medical school. before transferring the patient to the cath facility.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content