This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background Heart failure with preserved ejection fraction is a recognised outcome in patients with myocardialinfarction, although heart failure with reduced ejection fraction is more common. Among patients with myocardialinfarction, a 1-SD increase in pulse pressure was associated with a 1.60-fold m/s had a 2.10-fold
Heart failure (HF) is one of the significant complications in patients with myocardialinfarction (MI), leading to increased risk for cardiovascular morbidity and mortality. 2 However, mortality rate is greater in HF cases developing >3 days following MI compared with less than or equal to 3 days after MI.
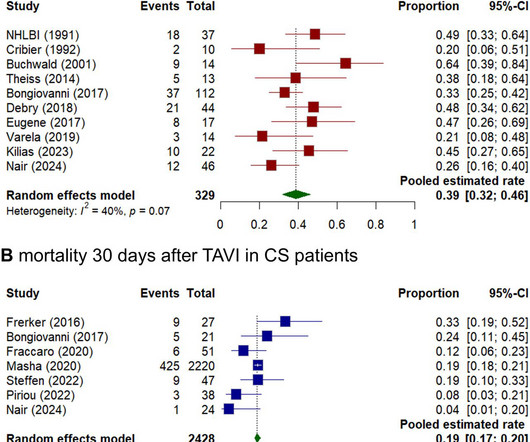
Background Cardiogenic shock (CS) induced by severe aortic stenosis (AS) is a life-threatening condition with high mortality. Aim This study aimed to systematically review and analyse the existing evidence on outcomes of emergency transcatheter aortic valve implantation (eTAVI) and emergency balloon aortic valvuloplasty (eBAV) in CS patients.
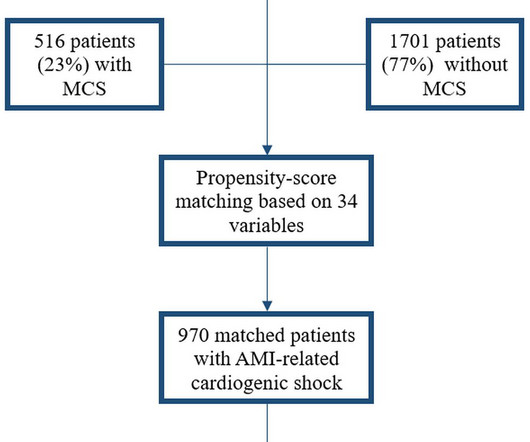
Background Despite limited beneficial evidence, mechanical circulatory support (MCS) is commonly used in patients with acute myocardialinfarction-related cardiogenic shock (AMI-CS). MCS was deployed in 516 patients (23.3%), of which the intra-aortic balloon pump was used most frequently (n=253, 49.0%).
Small aortic annulus poses a major challenge in aortic valve replacement due to the increased risk of prosthesispatient mismatch (PPM) and increased surgical risk. In recent years, transcatheter aortic valve replacement (TAVR) has emerged as a popular alternative to the traditional surgical aortic valve replacement.
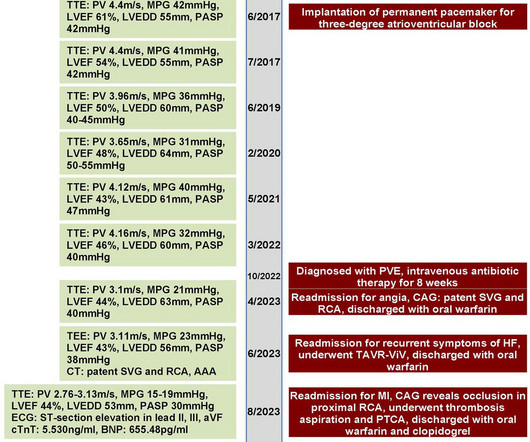
A 70-year-old female patient with a history of bioprosthetic aortic valve replacement and coronary artery bypass graft presented with bioprosthetic valve failure secondary to prosthetic valve endocarditis. This resulted in early death due to myocardialinfarction and acute heart failure.
The NOTION trial, a pioneering study, sought to compare the long-term clinical and bioprosthesis outcomes of Transcatheter Aortic Valve Implantation (TAVI) versus Surgical Aortic Valve Replacement (SAVR) in patients with severe aortic valve stenosis (AS) at lower surgical risk. Severe SVD was defined by specific criteria.
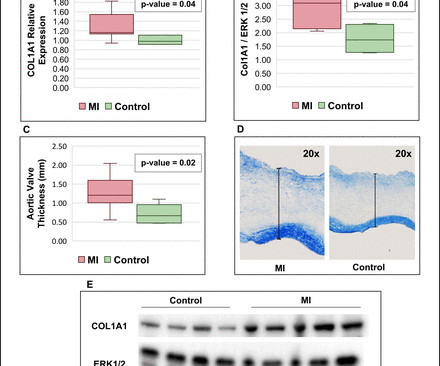
Background Myocardialinfarction (MI) has been shown to induce fibrotic remodelling of the mitral and tricuspid valves. It is unknown whether MI also induces pathological remodelling of the aortic valve and alters aortic stenosis (AS) progression. vs –0.04±0.04 cm 2 /m 2 /year; p=0.004).
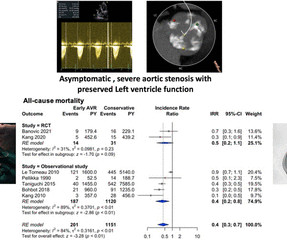
Background A quarter of patients with severe aortic stenosis (AS) were asymptomatic, and only a third of them survived at the end of 4 years. Only a select subset of these patients was recommended for aortic valve replacement (AVR) by the current American College of Cardiology/American Heart Association guidelines.
Aortic dissection is a severe cardiovascular condition associated with high mortality rates, particularly in cases of Stanford type A aortic dissection (TAAD). Myocardialinfarction with non-obstructive corona.
Prosthetic valve thrombosis (PVT) in aortic valve and its complication coronary embolism is a very rare condition. We present a young patient with acute myocardi. Diagnosis and treatment process is challenging.
Background Redo sternotomy aortic root surgery is technically demanding, and the evidence on outcomes is mostly from retrospective, small sample, single-centre studies. We report the trend, early clinical results and outcome predictors of redo aortic root replacement over 20 years in the United Kingdom. Age >59 (OR: 2.99, CI: 1.92–4.65,
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
Publication date: Available online 17 December 2024 Source: The American Journal of Cardiology Author(s): Ariane Lemieux, Helen Hashemi, Charles S. Roberts, Jeffrey M. Schussler
BackgroundProtruding aortic plaque is known to be associated with an increased risk for future cardiac and cerebrovascular events. Coronary plaque characteristics were compared to evaluate coronary plaque vulnerability in patients with protruding aortic plaque on computed tomography angiography.
BackgroundLp(a) (lipoprotein(a)) is an independent risk factor for calcific aortic valve stenosis (CAVS). Journal of the American Heart Association, Ahead of Print. Whether patients with CAVS and high Lp(a) levels are at higher risk of valvular or cardiovascular events is unknown.
This study aimed to confirm the prognostic value of a novel angiographic microvascular resistance (AMR) index in patients undergoing transcatheter aortic valve replacement.Methods and ResultsWe prospectively included 335 patients with severe aortic stenosis who underwent transcatheter aortic valve replacement at Fuwai Hospital.
This potential vascular market for this product family is measured in millions of procedures per year, including cardiac interventions such as structural heart procedures and electrophysiology procedures, peripheral vascular interventions including renal interventions, endovascular aortic repair, and carotid artery interventions.
The kappa was higher in MA versus FFS for diabetes (P=0.03) and hypertension (P=0.025) but was lower in myocardialinfarction (P<0.0001). For the outcomes, sensitivities were 85% for bleeding (comprehensive), permanent pacemaker implantation, and death.
Background and aims Randomised controlled trials comparing transcatheter aortic valve replacement (TAVR) and surgical aortic valve replacement (SAVR) were performed in highly selected populations and data regarding long-term secondary complications beyond mortality are scarce. All-cause mortality at 1 year (HR 1.21; 95% CI 1.02
BackgroundCurrent guidelines and expert consensus recommend lifelong single antiplatelet therapy for patients undergoing transcatheter aortic valve replacement who have no indication for anticoagulation or dual antiplatelet therapy. Journal of the American Heart Association, Ahead of Print.
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardialinfarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). Mechanical complications secondary to myocardialinfarction are infrequent due to most patients receiving revascularization quite rapidly.
Objective The optimal medical therapy after surgical aortic valve replacement (SAVR) for aortic stenosis remains unknown. Methods All patients undergoing SAVR due to aortic stenosis in Sweden 2006–2020 and surviving 6 months after surgery were included.
We report a 42-year-old male patient who was diagnosed with acute myocardialinfarction (AMI), and subsequently underwent percutaneous coronary intervention (PCI) for revascularization. The patient was transferred to the cardiac intensive care unit for intra-aortic balloon pump (IABP) due to frequent malignant arrhythmia after PCI.
Abstract: Transcatheter aortic valve replacement (TAVR) is an interventional procedure performed in patients with severe aortic stenosis and often required perioperative antiplatelet therapy. There were no significant differences in the incidence of other bleeding events, transfusions, stroke, myocardialinfarction, or all-cause death.
Introduction Compared with first-line antihypertensives, beta-blockers (BB) have been reported to lower the central aortic blood pressure suboptimally and are associated with increased stroke risk. Similarly, the risk of total myocardialinfarction was 1.76 mmHg [95% confidence interval (CI):1.16–2.33; mmHg (95% CI: 0.86–3.00;
Objective Postprocedural ischaemic and bleeding risks after transcatheter aortic valve replacement (TAVR) remain a major concern. Ischaemic events were defined as myocardialinfarction, stroke, transient ischaemic attack or peripheral embolism at 1 year.
The primary outcome was ischemic stroke; the secondary outcome was combined cardiovascular events (ischemic stroke, myocardialinfarction, and cardiovascular death). years, 236 (25.3%) cardiovascular events occurred (76 ischemic strokes, 27 myocardialinfarctions, and 133 cardiovascular deaths).
Previous medical interventions included a spectrum of procedures, including catheter-directed thrombectomy for popliteal artery aneurysms with thrombosis, vascular bypass grafting for cerebral-anterior communicating artery aneurysms and arch replacement and stent implantation for aortic dissecting aneurysms.
Background:Atherosclerotic cardiovascular disease (ASCVD) is highly prevalent in patients with severe aortic stenosis undergoing transcatheter aortic valve replacement (TAVR). Circulation: Cardiovascular Interventions, Ahead of Print. Exposure of interest was PVD. Primary outcome was all-cause mortality.
A 53-year-old male presenting emergently with signs of myocardialinfarction received immediate coronary angiography and thoracic CT-scan showing occlusion of the first marginal coronary branch without possibility of revascularization and minimal pericardial extravasation.
Objectives:The aim of this study was to assess the risk of stroke for temporary mechanical circulatory support (tMCS) device treated acute myocardialinfarction (AMI).Background:Data Background:Data are limited regarding risk of stroke for temporary mechanical circulatory support (tMCS) device treated acute myocardialinfarction (AMI).Methods:The
It is now well known that even if a coronary artery is opened well after a myocardialinfarction, with good flow in the epicardial coronary arteries, there could be impaired myocardial perfusion. Prognostic Value of Microvascular Resistance Reserve After Percutaneous Coronary Intervention in Patients With MyocardialInfarction.
Variables and prognosis were analysed based on the presence or absence of NCA, defined as previous stroke, transient ischaemic attack (TIA), or peripheral artery disease (PAD) [lower extremity artery disease (LEAD), carotid disease, previous lower limb vascular surgery, or abdominal aortic aneurysm (AAA)].
They also wanted an aortic CT which was negative. Timing of revascularization in patients with transient ST segment elevation myocardialinfarction: a randomized clinical trial. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. This is a "Transient OMI".
The Queen of Hearts disagrees, diagnosing OMI with high confidence: Case Continued: The EKG was not immediately recognized by the emergency provider, who ordered a CT scan to rule out aortic dissection at 1419. Diagnosis of Type I vs. Type II MyocardialInfarction in Emergency Department patients with Ischemic Symptoms (abstract 102).
In the early years of percutaneous coronary intervention (PCI), studies indicated a heightened risk of major adverse cardiac events (MACE) in patients with reduced left ventricular ejection fraction (LVEF), involving outcomes such as death, Q-wave myocardialinfarction (MI), stent thrombosis, and repeat revascularization.
FFR is obtained by dividing the pressure distal to the stenosis by the central aortic pressure, which is usually equal to the pressure proximal to the stenosis if there is no additional stenosis in between. They had lower rates of mortality or myocardialinfarction. myocardialinfarction rate and 3.2% or less.
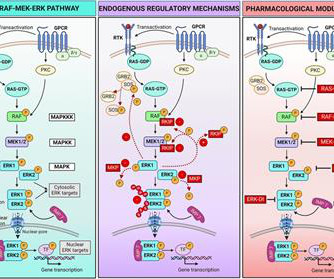
We then summarize current knowledge of the roles played by ERK in the development and progression of cardiac and vascular disorders, including atherosclerosis, myocardialinfarction, cardiac hypertrophy, heart failure, and aortic aneurysm.
BACKGROUND:Food and Drug Administrationmandated postmarket studies for transcatheter aortic valve replacement in low-risk populations plan to use passively collected registry data linked to claims for long-term follow-up out to 10 years. Circulation: Cardiovascular Interventions, Volume 18, Issue 1 , Page e014592, January 1, 2025.
EMPACT-MI 1 ( NCT04509674 ) studied the effects of empagliflozin in patients who have experienced myocardialinfarction (MI). SMART 4 ( NCT04722250 ) studied patients with severe aortic stenosis and a small aortic annulus who underwent transcatheter aortic valve replacement (TAVR). vs. 6.2%) and stroke (2.9%
to 8.34; 4.27), myocardialinfarction (69.6; to 6.85; 4.54), aortic stenosis (18.7; Higher-predicted risk, compared with lower-predicted risk, was associated with incident chronic kidney disease (cumulative incidence per 1000 persons at 10 years 245.2; HR 6.85, 95% CI 6.70 to 7.00; median time to event 5.44 12.54, 12.08
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content