This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This EKG is diagnostic of transmural ischemia of the inferior wall. The Queen of Hearts disagrees, diagnosing OMI with high confidence: Case Continued: The EKG was not immediately recognized by the emergency provider, who ordered a CT scan to rule out aortic dissection at 1419. Lead I also shows reciprocal ST depression. Smith SW.
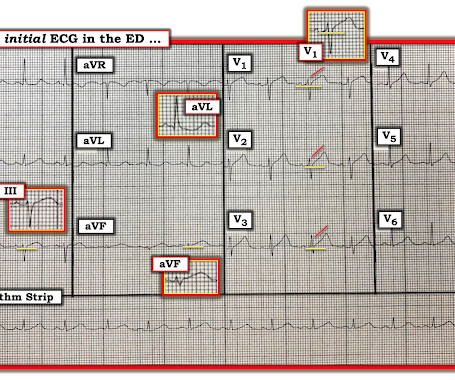
He interprets here: "This EKG is diagnostic of right bundle branch block and transmural ischemia of the anterior wall, most likely from an occlusion of the proximal LAD. The provider had sent the patient for an aortic dissection scan which had shown extremely heavy calcification of the LAD. It was recorded at 0530: What do you think?
Look at the aortic outflow tract. Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve.
There is profound LVH with anterolateral ST elevation and reciprocal ST depression in II, III, aVF, and ST depression in V5 and V6 that could all be secondary to LVH or could represent ischemia superimposed on the repolarization abnormalities of LVH: note that wherever there is ST depression, it is associated with a very high voltage R-wave.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.”
Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. and repeat the ECG, to see if the apparent ischemia persists. A third ECG was done about 25 minutes after the first: This shows resolution of all apparent ischemia.
Left ventricular afterload reduction is essential to decrease the trans-se ptal pressure gradient and thus decrease shunt volume, making a larger proportion of the blood flow from the left ventricle through the aortic valve. A mong patients with STEMI, ventricular septal rupture is the most common and free wall rupture is the least common.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. Two weeks ago he had a significant MVC with many severe injuries, including aortic injury s/p endovascular repair. I sent this to our group without information and Dr. Smith responded: "Not OMI.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
Part of the ST depression with deep T wave inversion in the lateral chest leads clearly reflects LV "strain" from the marked LVH — but despite the very large QRS amplitudes, this ST-T wave appearance looks disproportionate, suggesting at least a component of ischemia. The plan was to proceed as soon as possible with aortic valve replacement.
It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. An elderly patient with a ruptured abdominal aortic aneurysm: Formal ECG Interpretation (final read in the chart!) : "Inferior ST elevation, lead III, with reciprocal ST depression in aVL."
There is ventricular hypertrophy in the absence of abnormal loading conditions, such as aortic stenosis, or hypertension, for example – of which the most common variant is Asymmetric Septal Hypertrophy. There is LBBB-like morphology with persistent patterns of subendocardial ischemia.
The patient arrived looking like an aortic dissection patient, so CTA was done and negative." Resolution of pain, by itself, is not reliable enough to be certain of resolution of ischemia. the ischemia has truly resolved. OMI often does not meet STEMI criteria. ST elevation at 60 ms after the J-point in lead V3 = 1.5
A repeat ECG was done: Obvious anterolateral wall STEMI. On arrival his BP was 70s/40s, so an intra-aortic ballon pump was placed. This means that they occur shortly after onset of occlusion, but also may be the last remaining sign of ischemia after ST elevation resolves (after reperfusion).
50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. CT angiogram chest: no aortic dissection or pulmonary embolism. 24 yo woman with chest pain: Is this STEMI?
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. An EKG from a year prior was available for comparison: The ED physician noted Initial EKG here read by the computer as a STEMI, however, there is a very poor baseline and a lot of artifact. See reference and discussion below.
Ischemia often produces a straightening of the ST segment and sometimes upward convexity. That said — the overall picture to me did not "look" acute — and the history of "chest pain radiating to the back " in this 80-something man with marked LVH — made me strongly consider an aortic dissection as a more likely cause.
His initial high sensitivity troponin I returned at 1300 ng/L and given that his cardiac workup was otherwise unremarkable, a CT was obtained to evaluate for pulmonary embolism and aortic aneurysm or dissection but this too was unrevealing. Another EKG was also obtained. ECG at time 82 minutes: What do you think?
50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). There were no other causes of dyspnea apparent and thus we can assume that myocardial ischemia started 6 days prior. See Raitt et al.:
It is diagnostic of OMI, but this is SUBACUTE OMI I sent this ECG to my "EKG Nerdz" friends, without any clinical info at all and they answered "OMI" The Queen said: "STEMI-Equivalent with High Confidence:" Notice she sees findings in both normal beats and PVCs. If this were ACUTE (vs. Regional wall motion abnormality--mid anterior akinesis.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content