This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Food and Drug Administration ( FDA ) announced that Teleflex , and their subsidiary Arrow International , are recalling the Arrow FiberOptix Intra-Aortic Balloon Catheter Kit and Arrow UltraFlex Intra-Aortic Balloon Catheter Kits after finding that a manufacturing error may cause the catheter’s balloon to become overtwisted.
ObjectiveSpinal cord ischemia due to damage or occlusion of the orifices of aortic segmental arteries (ASA) is a serious complication of open and endovascular aortic repair. Furthermore, it aids in planning and conducting safe aortic intervention and assists in deciding on single- or two-staged stent graft procedures.
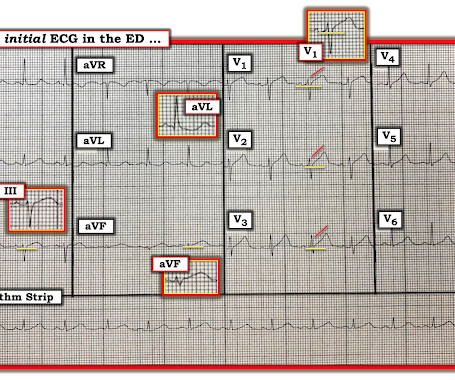
This EKG is diagnostic of transmural ischemia of the inferior wall. The Queen of Hearts disagrees, diagnosing OMI with high confidence: Case Continued: The EKG was not immediately recognized by the emergency provider, who ordered a CT scan to rule out aortic dissection at 1419. Lead I also shows reciprocal ST depression.
Many of the changes seen are reminiscent of LVH with “strain,” and downstream Echo may very well corroborate such a suspicion, but since the ECG isn’t the best tool for definitively establishing the presence of LVH, we must favor a subendocardial ischemia pattern, instead. Type I ischemia. Type II ischemia.
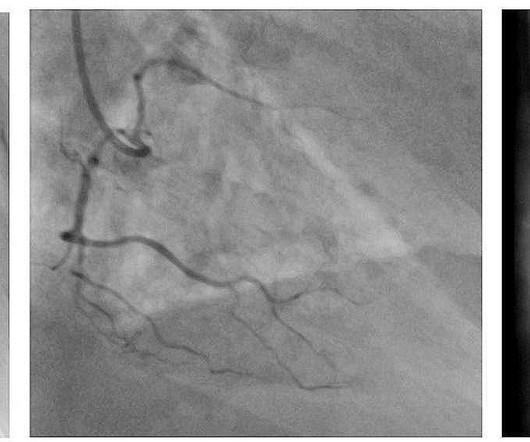
Look at the aortic outflow tract. The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Aortic angiogram did not reveal aortic dissection. What do you see? Answer below in the still shot.
Objective The initial operation for type A aortic dissection has limitations, and there may be a need for reoperation in cases such as giant pseudoaneurysm formation and reduced blood supply to the distal vessels. In this study, we retrospectively analyzed the recorded data of 62 patients.
Background Surgery for type A aortic dissection (TAAD) is associated with high risk of mortality. Methods Subjects were patients who underwent surgery for acute TAAD at 18 European centers of cardiac surgery from the European Registry of Type A Aortic Dissection (ERTAAD). Current risk scoring methods have a limited predictive accuracy.
Transcatheter aortic valve replacement (TAVR) is increasing in popularity for symptomatic severe aortic stenosis. Transfemoral arterial route is the most commonly used approach for TAVR, also known as TAVI or transcatheter aortic valve implantation. No calcifications in the artery causing vascular stenosis. JACC: Asia.
The second case is a 76-year old male brought to the emergency room after sudden syncope, clinical sings of pericardial tamponade and suspicion of a type A acute aortic dissection. Immediate sternotomy under mechanical resuscitation enabled removal of the massive intrapericardial clot and revealed LVFWR.
IntroductionAcute spinal cord ischemia syndrome (ASCIS) is a rare disease that is thought to comprise roughly only 1.2% A diagnostic spinal angiogram was completed with no evidence of arteriovenous fistula or aortic dissection. Stroke: Vascular and Interventional Neurology, Volume 3, Issue S2 , November 1, 2023. of all strokes [1, 2].
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
He interprets here: "This EKG is diagnostic of right bundle branch block and transmural ischemia of the anterior wall, most likely from an occlusion of the proximal LAD. The provider had sent the patient for an aortic dissection scan which had shown extremely heavy calcification of the LAD. It was recorded at 0530: What do you think?
There is profound LVH with anterolateral ST elevation and reciprocal ST depression in II, III, aVF, and ST depression in V5 and V6 that could all be secondary to LVH or could represent ischemia superimposed on the repolarization abnormalities of LVH: note that wherever there is ST depression, it is associated with a very high voltage R-wave.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m. ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
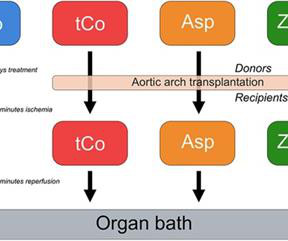
The degree of ischemia-reperfusion injury (IRI), which occurs during the harvest and implantation of the grafts, is an important determinant of graft patency. There was also a non-ischemia-reperfusion control group ( n = 8). Introduction Coronary artery bypass grafting (CABG) is the most common cardiac surgical procedure.
The differential is: Posterolateral OMI or subendocardial ischemia The distinction between posterior OMI and subendocardial ischemia can be important and sometimes difficult. A dissection flap is noted in the intrabdominal aorta, and the aortic outflow tract is also noted to appear wider than normal.
Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. and repeat the ECG, to see if the apparent ischemia persists. A third ECG was done about 25 minutes after the first: This shows resolution of all apparent ischemia.
It should be known that each category can easily manifest the generic subendocardial ischemia pattern. In general, subendocardial ischemia is a consequence of global supply-demand mismatch that usually ameliorates upon addressing, and mitigating, the underlying cause. What’s interesting is that the ECG can only detect ischemia.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
Two weeks ago he had a significant MVC with many severe injuries, including aortic injury s/p endovascular repair. That said — I did not interpret these differences as the result of acute ischemia. Context: a man in his 40s presented to the emergency department with 1 day of sudden onset chest pain.
Part of the ST depression with deep T wave inversion in the lateral chest leads clearly reflects LV "strain" from the marked LVH — but despite the very large QRS amplitudes, this ST-T wave appearance looks disproportionate, suggesting at least a component of ischemia. The plan was to proceed as soon as possible with aortic valve replacement.
FFR is obtained by dividing the pressure distal to the stenosis by the central aortic pressure, which is usually equal to the pressure proximal to the stenosis if there is no additional stenosis in between. indicates inducible ischemia while an FFR above 0.80 excludes ischemia in 90% of cases. Normal FFR is 1.0 An FFR below 0.75
Written by Pendell Meyers A woman in her 20s with connective tissue disorder and history of aortic root and valve repair presented with palpitations. Further history revealed she had new onset atrial flutter soon after her aortic surgery, and was put on flecainide approximately 1 month ago. Here is her triage ECG: What do you think?
Left ventricular afterload reduction is essential to decrease the trans-se ptal pressure gradient and thus decrease shunt volume, making a larger proportion of the blood flow from the left ventricle through the aortic valve. Surgical repair of the VSR was eventually done.
The two groups exhibited similar patient characteristics, anatomical factors including aortic arch, and clinical outcomes. Left TRA may offer a safer and more reliable approach for various aortic arch configurations and for both right- and left-sided carotid lesions. years, 83.7%, and 53.5% in the right TRA group, and 74.8
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
Given radiation of pain into the patient's back, he underwent CTA which showed no evidence of aortic dissection or any other acute pathology. and morphine 4 mg IV ( Smith : this is even more worthless, and just hides the fact that the patient is having ongoing ischemia and infarction) , and repeat ECG was obtained.
remain hypo- or akinetic for some time even if not infarcted, just due to the profound ischemia incurred during the occlusive phase. Thus, an acute wall motion abnormality is not a sign of active or persistent ischemia, and thus is not necessarily an indication for emergent cath. Even many NOMI have wall motion abnormalities.
Then, in PDA Eisenmenger, you can have aortic enlargement because the shunt is received in the aortopulmonary region, aorta can be enlarged in PDA Eisenmenger. In VSD Eisenmenger, there is no aortic enlargement, there is no cardiomegaly. And it was described from the very first report of Eisenmenger syndrome.
2] Here there is no posterior ST elevation, but the anterior ST depression is also less—so it is dynamic, confirming acute ischemia. The absence of STE in V7-V9 is often due to resolution of ischemia, as seen by resolution of ST depression in V7-V9. But it is still STEMI negative.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Chest trauma was suspected on initial exam. Here is his initial ECG around 1330: What do you think?
There is ventricular hypertrophy in the absence of abnormal loading conditions, such as aortic stenosis, or hypertension, for example – of which the most common variant is Asymmetric Septal Hypertrophy. There is LBBB-like morphology with persistent patterns of subendocardial ischemia.
The patient arrived looking like an aortic dissection patient, so CTA was done and negative." Resolution of pain, by itself, is not reliable enough to be certain of resolution of ischemia. the ischemia has truly resolved. ST elevation at 60 ms after the J-point in lead V3 = 1.5 and thus indicating LAD occlusion).
The first troponin returned at 0.099 ng/mL (elevated, consistent with Non-Occlusion MI) Providers were concerned with aortic dissection, so they order a chest aorta CT. This transmural ischemia, but not necessarily completed infarction (yet).
An elderly patient with a ruptured abdominal aortic aneurysm: Formal ECG Interpretation (final read in the chart!) : "Inferior ST elevation, lead III, with reciprocal ST depression in aVL." Is there likely to be fixed coronary stenosis that led to demand ischemia during pneumonia? --Was What do you think? Does he need a stress test? --Is
On arrival his BP was 70s/40s, so an intra-aortic ballon pump was placed. This means that they occur shortly after onset of occlusion, but also may be the last remaining sign of ischemia after ST elevation resolves (after reperfusion). A repeat ECG was done: Obvious anterolateral wall STEMI.
There was concern for aortic dissection, so a CT was done and was negative. For coronary anatomy, see here: [link] This is the post intervention ECG: All ST Elevation is gone (more proof that it was all a result of ischemia) Formal Echo: Normal estimated left ventricular ejection fraction - 55%. It was stented. Learning Points: 1.
1,2 ASCVD causes or contributes to conditions that include coronary artery disease (CAD), cerebrovascular disease, and peripheral vascular disease (inclusive of aortic aneurysm).3 mg reduced the risk of cardiovascular death, MI or heart attack, ischemic stroke, or ischemia-driven coronary revascularization by 31% compared with placebo.34
These include ( among others ) — acute febrile illness — variations in autonomic tone — hypothermia — ischemia-infarction — malignant arrhythmias — cardiac arrest — and especially Hyperkalemia. Patients with such conditions that may transiently mimic the ECG findings of a Brugada-1 pattern are said to have Brugada Phenocopy.
CT angiogram chest: no aortic dissection or pulmonary embolism. He spent several days in the PICU, undergoing workup including: Serial troponins: rising from 5,700 ng/L (unknown if I or T) to greater than 25,000 ng/L (greater than the lab's upper limit of reporting). No further troponins were measured.
Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Evidence of acute ischemia (may be subtle) vii. heart auscultation (aortic stenosis); c. 2nd or 3rd degree AV blocks or sinus pause of at least 2 seconds iv. Right bundle branch block (BBB) with hemiblock (bifascicular block) v. Left BBB vi. LVH or RV d.
But it also shows a massive area of total ischemia in the LAD territory: CT shows the infarct The CT is with contrast, which increases density (which looks more white). Important: It is exceedingly rare for an anterior STEMI to be due to Aortic Dissection. Here it is: Type A Aortic Dissection Why was the troponin so elevated?
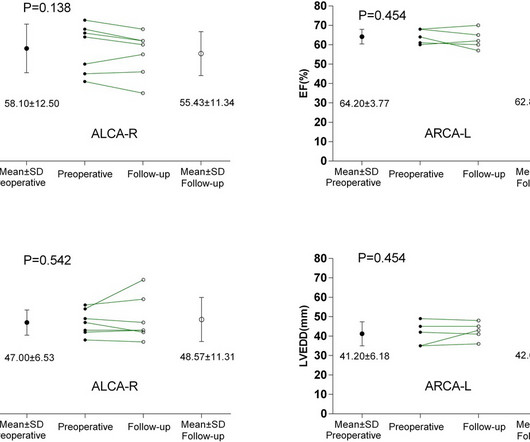
BackgroundAnomalous aortic origin of a coronary artery (AAOCA) is associated with an increased risk of myocardial ischemia and sudden cardiac death. ResultsThe median age at surgery was 26 years (range, 13–57 years).
The patient was started on heparin for possible NSTEMI vs demand ischemia. Smith : "decompensation" of aortic stenosis might have initiated this entire cascade. Smith : "decompensation" of aortic stenosis might have initiated this entire cascade. What "initiates" the aortic stenosis cascade?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content