This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Fetal aortic valvuloplasty is considered for fetuses with severe valvar aortic stenosis and echocardiographic features suggesting a risk of progression to hypoplastic left heart syndrome. So if progression to hypoplastic left heart syndrome can be prevented by fetal aortic valvuloplasty, that would be theoretically a great boon.
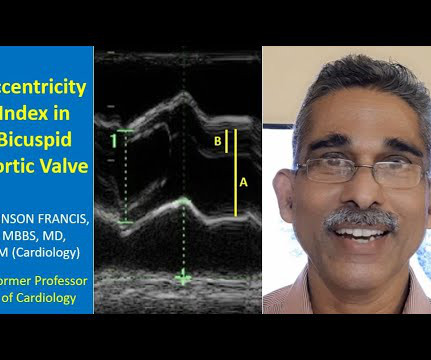
Transcript of the video: Closure line of aortic valve on M-Mode echocardiogram, is seen as central line, while in bicuspid aortic valve, it is an eccentric closure, nearer to one of the walls of the aorta. This eccentricity of closure of the aortic valve leaflets, can be calculated using what is known as eccentricity index.
The large aortic regurgitation jet can be seen as a mosaic jet in the left ventricular outflow tract anterior to the anterior mitral leaflet. A portion of the thickened aortic valve can be seen between the aorta and left ventricle. Thickening of both aortic and mitral leaflets indicate the possible etiology as rheumatic.
You can see the reverse flow into the left ventricle from the aorta, with the aortic valve in closed position. Beacuse, as the aortic valve is closed, and the regurgitant jet is coming in, and left ventricular diastolic pressures are lower than the aortic pressures. You cannot say its highly quantitative estimation.
This is reverse flow from the aortic valve, that is aortic regurgitation jet. That is, flow away from the transducer is depicted as blue. Flow towards the transducer is depicted as red. Here, this is the forward flow through the mitral valve in diastole in red. That also occurs in diastole.
Transcatheter aortic valve replacement (TAVR) is increasing in popularity for symptomatic severe aortic stenosis. Transfemoral arterial route is the most commonly used approach for TAVR, also known as TAVI or transcatheter aortic valve implantation. JACC: Asia. May 14, 2024. Epublished DOI: 10.1016/j.jacasi.2024.03.006
The optimal management of concomitant chronic obstructive coronary artery disease (CAD) in transcatheter aortic valve replacement (TAVR) recipients remains a debated topic. While some advocate for pre-TAVR percutaneous coronary intervention, others adopt an expectant approach.
Locomotor brachii or locomotor brachialis is often described as a peripheral sign in severe aortic regurgitation or other causes of aortic runoff. The post Locomotor Brachii appeared first on All About Cardiovascular System and Disorders.
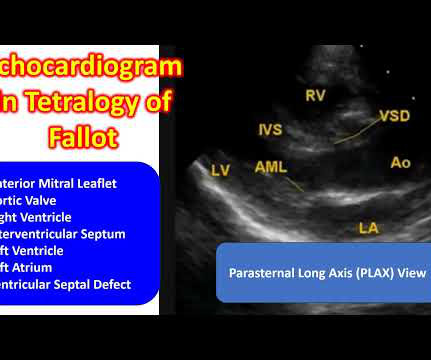
This is the aortic valve in closed position and mitral valve also appears to be closed in position. You can also see the aortic override. So, when there is an aortic override, if the override of the aorta is less than 50%, you think of tetralogy of Fallot. Separation between the attachments of the aortic and mitral valve.
Unlike the valves on the left side like the mitral and aortic, right sided valves can have some leak. That is, mild mitral regurgitation and mild aortic regurgitation are less common. But even in nearly normal persons, there could be a little bit of leak in the tricuspid valve. That is known as mild tricuspid regurgitation.
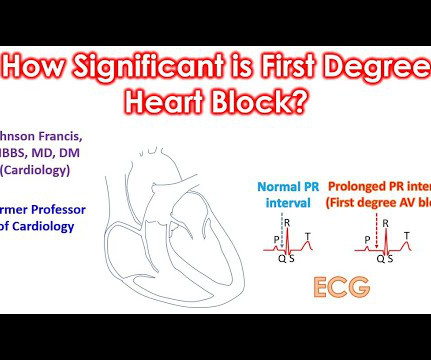
Calcium deposits in the aortic valve between the left ventricle, the lower left chamber and the aorta which receives the blood pumped out, can spread to the conduction system and produce first degree AV block. First degree AV block in older persons due to degeneration of the conduction system or aortic valve can also progress.
Microvascular resistance evaluated whether the vasodilatory reserve capacity of coronary microcirculation was restored in the infarcted territory, regardless of concomitant epicardial coronary artery disease and aortic pressure.
Devices like an intra-aortic balloon pump and left ventricular assist device may be useful to some extent. Intra-aortic balloon pump uses intermittent inflation of a balloon attached to a tube placed in the aorta. Medications are given as a drip to enhance the blood pressure as an emergency measure.
This is reverse flow from the aortic valve, that is aortic regurgitation jet. That is, flow away from the transducer is depicted as blue. Flow towards the transducer is depicted as red. Here, this is the forward flow through the mitral valve in diastole in red. That also occurs in diastole.
SMART 4 ( NCT04722250 ) studied patients with severe aortic stenosis and a small aortic annulus who underwent transcatheter aortic valve replacement (TAVR). The study concluded that among low-risk patients with severe aortic stenosis, TAVI is as effective as SAVR in terms of the composite outcome of death or stroke at 1 year.
In this image, aortic regurgitation jet is seen as aliased, with part of it above the baseline and part of it below the baseline, which is known as wrap around. It is shown as a circle along the dotted Doppler line in the image, just beyond the aortic valve. Nyquist limit is half the pulse repetition frequency.
Transcript of video: Hypoplastic Left Heart Syndrome is a very severe form of congenital heart disease, in which, the left ventricle, aorta and mitral and aortic valves are hypoplastic and valves may be atretic as well. It has a very poor survival. This is diagrammatic representation of hypoplastic left heart syndrome.
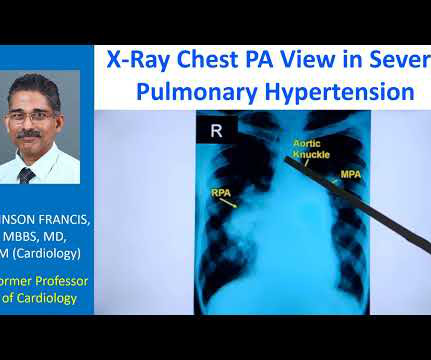
This is the aortic knuckle. In PDA Eisenmenger, there will be more prominence of aortic knuckle shadow is expected in PDA Eisenmenger and another finding which you would expect in long standing PDA Eisenmenger would be calcification of the ductus, as an inverted Y shadow in this region. It is not visible here.
Another important serious disease which has to be thought of in a person with pain in the chest or upper back is aortic dissection. Aortic dissection is tear in the inner lining of the aorta. Difference in blood pressure between the arms is more likely in the presence of risk factors.
FFR is obtained by dividing the pressure distal to the stenosis by the central aortic pressure, which is usually equal to the pressure proximal to the stenosis if there is no additional stenosis in between. Matching of the wire tip pressure and the aortic pressure should be done before crossing the lesion. Normal FFR is 1.0
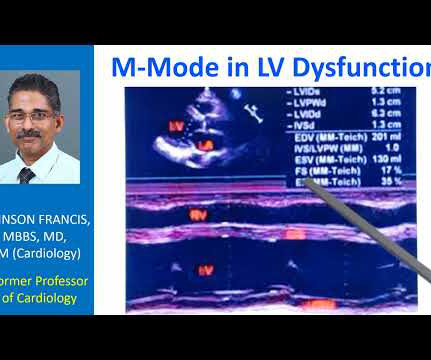
Right ventricular outflow tract, left ventricle, left atrium, aorta, aortic valve, mitral valve. In the inset you can see the two dimensional image. Location of the transducer here, in the parasternal region. This is the parasternal long axis view. These are the things you have seen in that inset image.
You can see the ventricular septal defect and aortic over ride. And, usually this done, Blalock-Taussig shunt, classic shunt, opposite to the side of the aortic arch. There are several surgical options for tetralogy of Fallot and also some sequelae for these, we will see. This is the diagrammatic representation of tetralogy of Fallot.
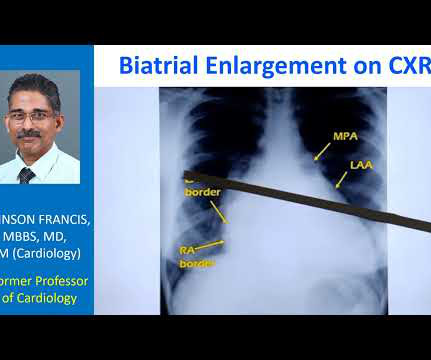
When there are bulges, aortic knuckle is first mogul, main pulmonary artery segment is second mogul, and left atrial appendage is taken as the third mogul sign. When there is gross pulmonary hypertension, instead of these being straight over here, it will form a bulge over here.
Then, in PDA Eisenmenger, you can have aortic enlargement because the shunt is received in the aortopulmonary region, aorta can be enlarged in PDA Eisenmenger. In VSD Eisenmenger, there is no aortic enlargement, there is no cardiomegaly.
Pain of aortic dissection is tearing type and is most severe in the beginning. A still rare, but very dangerous condition is breaks in the inner lining of the aorta, the largest blood vessel supplying oxygenated blood to the whole body.
Usual structures imaged in this view are the right ventricular free wall and outflow region, interventricular septum, aorta, and aortic valve, left ventricular outflow tract, anterior and posterior mitral leaflets, left ventricular cavity, posterior wall of left ventricle and left atrium. Gradient of coarctation can be assessed in this view.
Doing a fenestration during lateral tunnel type of repair was quite easy while doing it during extra cardiac conduit placement was ‘annoying’ During an extra cardiac conduit placement, placing a fenestration would mean aortic cross clamping and stopping the heart for placing a fenestration.
So it will not produce a true LV to aorta pullback tracing, which is required in cases like aortic stenosis. When the tip is in the left ventricle, this region will be in the aorta sometimes. For that you will have to use a catheter without side holes like this, like a multi-purpose catheter or some other catheter you have to use.
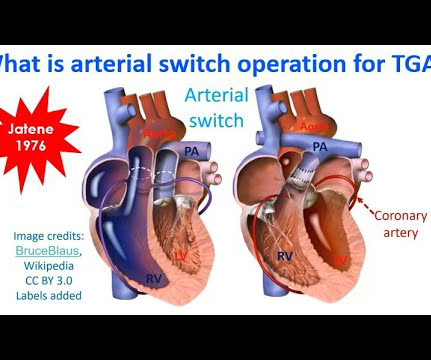
There could be enlargement of aorta, neoaorta, producing annuloaortic ectasia and aortic regurgitation, another long term sequelae of arterial switch operation. This is diagrammatic representation of another of the complications, delayed sequelae of arterial switch.
Rare long term problems include narrowing of the pulmonary artery and aortic regurgitation due to aortic root enlargement. I has to be done quite early in life before the left ventricular muscle mass regressed due to the lower load of the pulmonary circulation. Delayed surgery has been undertaken with ECMO support in some cases.
Right ventricle is an anterior structure and aortic root is relatively posterior to it, and hence the anteroposterior flow depicted in blue colour. Parasternal long axis view showing colour flow from right ventricle to aorta through the ventricular septal defect with overriding aorta.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content