This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
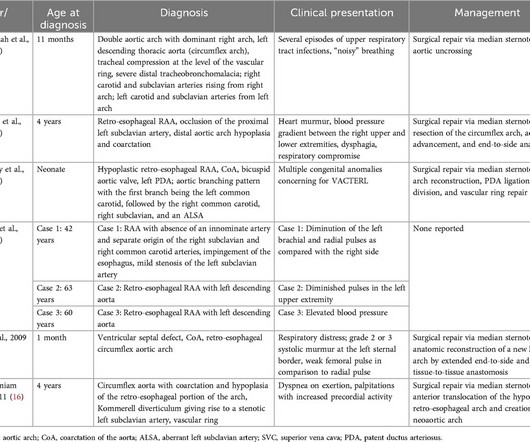
Circumflex right aortic arch is a rare aortic arch anomaly where the arch extends in a retro-esophageal pattern with a left-sided descending thoracic aorta. A 33-year-old G4P3 patient underwent fetal echocardiography after obstetric ultrasound showed concern for double aortic arch.
Cedars-Sinai and Smidt Heart Institute investigators developed a novel foundation model that integrates computer vision interpretation of echocardiogram images with natural language processing to augment cardiologists’ interpretation of echocardiograms. Image by Getty.
Food and Drug Administration (FDA) has granted 510(k) clearance for its first-of-a-kind, AI-powered AISAP CARDIO point-of-care ultrasound (POCUS) software platform. We know that structural heart disease and heart failure are the leading causes of hospitalization and morbidity in the U.S.
Serial echocardiographic assessments are common in clinical cardiology, e.g., for timing of intervention in mitral and aortic regurgitation. When following patients with serial echocardiograms, each new measur.
Blunt cardiac injury my result in : 1) Acute myocardial rupture with tamponade 2) Valve rupture (tricuspid, aortic, mitral) 3) Coronary thrombosis or dissection (and thus Acute MI) from direct coronary blunt injury 4) Dysrhythmias of all kinds. In the ED, ultrasound showed hemopericardium with tamponade.
Smith comment: This patient did not have a bedside ultrasound. Had one been done, it would have shown a feature that is apparent on this ultrasound (however, this patient's LV function would not be as good as in this clip): This is recorded with the LV on the right. Look at the aortic outflow tract. What do you see?
The next morning the patient went for his routine echocardiogram, where the operator noticed a dilated aortic root at 5.47 cm with severe aortic insufficiency. The team was notified and they ordered a stat aortagram which showed type A aortic dissection from the aortic valve to the iliacs. Pericarditis?
During echocardiography, a transducer transmits the ultrasound beam towards the heart. The image shown here is an animated 2 dimensional echocardiogram. This one is an older mode known as time-motion mode or M-Mode echocardiogram. Opening and closing movements of the aortic and mitral valves are visible.
An echocardiogram showed no hemopericardium, but D oppler showed a new small ventricular septal defect with left to right shunting. An intra-aortic balloon pump was placed, and the patient was taken for immediate surgical repair but did not survive. If detected early by ultrasound, the patient can be saved. 3) Oliva et al. (4)
See this case: what do you think the echocardiogram shows in this case? 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. Widespread ST-depression with reciprocal aVR ST-elevation can be cause by: Heart rate related: tachyarrhythmia (e.g., POCUS showed good LV-function and no pericardial effusion. Left main?
Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Check : [vitals, SOB, Chest Pain, Ultrasound] If the patient has Abdominal Pain, Chest Pain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). heart auscultation (aortic stenosis); c.
I suspect pulmonary edema, but we are not given information on presence of B-lines on bedside ultrasound, or CXR findings. Smith : "decompensation" of aortic stenosis might have initiated this entire cascade. What "initiates" the aortic stenosis cascade? Or I suspect that there is OMI simultaneous with another pathology.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content