This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
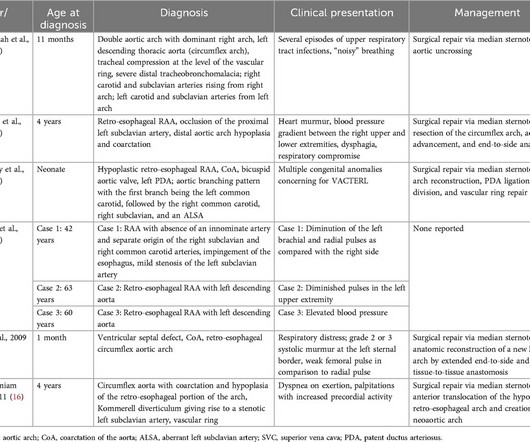
Circumflex right aortic arch is a rare aortic arch anomaly where the arch extends in a retro-esophageal pattern with a left-sided descending thoracic aorta. A 33-year-old G4P3 patient underwent fetal echocardiography after obstetric ultrasound showed concern for double aortic arch.
You can see the reverse flow into the left ventricle from the aorta, with the aortic valve in closed position. Beacuse, as the aortic valve is closed, and the regurgitant jet is coming in, and left ventricular diastolic pressures are lower than the aortic pressures. You cannot say its highly quantitative estimation.
Due to the chest pain radiating into the patient's back, the ER physician ordered CTA chest to rule out aortic dissection. This would have been fairly easy and much more expedient to diagnose with bedside echocardiogram. But seeing them all together is more suggestive that pericarditis could be possible.
Echocardiograms using the robotic arm resulted in the same diagnosis as conventional in-person echocardiography in 98% of cases (papillary muscle level obstruction was missed in one case). tim.hodson Thu, 08/29/2024 - 11:39 Aug. 28, 2024 — New research presented at this year’s ESC Congress 2024 in London, UK (Aug. 30 – Sept.
Transcript of the video: This is a still image from a colour Doppler echocardiogram, obtained from the apical five chamber view. This is reverse flow from the aortic valve, that is aortic regurgitation jet. These are the features, you have AR jet, and MR jet, in a still image of colour Doppler echocardiogram.
Cedars-Sinai and Smidt Heart Institute investigators developed a novel foundation model that integrates computer vision interpretation of echocardiogram images with natural language processing to augment cardiologists’ interpretation of echocardiograms. Image by Getty.
A transthoracic echocardiogram (TTE) revealed a mobile mass on the right coronary cusp of the aortic valve ( figure 1 , ). cm) at the right coronary cusp of the aortic valve on the long-axis and short-axis parasternal view. Figure 1 A mobile mass (1.88 Question What is the most likely diagnosis?
Transcript of the video: Closure line of aortic valve on M-Mode echocardiogram, is seen as central line, while in bicuspid aortic valve, it is an eccentric closure, nearer to one of the walls of the aorta. This eccentricity of closure of the aortic valve leaflets, can be calculated using what is known as eccentricity index.
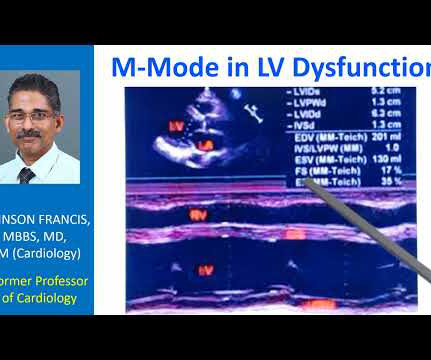
Transcript of the video: This is a still image of M-Mode Echocardiogram. Right ventricular outflow tract, left ventricle, left atrium, aorta, aortic valve, mitral valve. M-Mode is Time-Motion Mode. The horizontal axis is time. Vertical axis is distance from the transducer. In the inset you can see the two dimensional image.
The patient was managed medically and was referred to us in view of worsening symptoms with severe left ventricular dysfunction and moderate aortic regurgitation. Echocardiogram, CT aortogram and late gadolinium imaging of the aorta have been shown in figure 1. The coronary angiogram was normal.
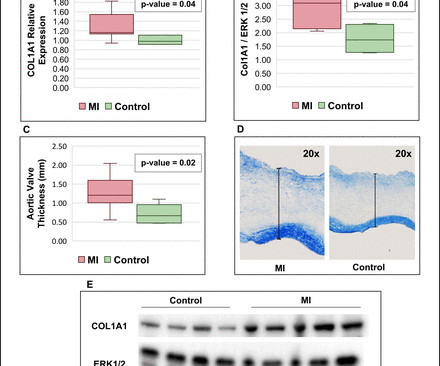
It is unknown whether MI also induces pathological remodelling of the aortic valve and alters aortic stenosis (AS) progression. We thus compared AS progression after an acute MI and in patients with/without history of MI, and assessed post-MI pathobiological changes within the aortic valve leaflets in a sheep model.
Transcript of the video: This is a still image from a colour Doppler echocardiogram, obtained from the apical five chamber view. This is reverse flow from the aortic valve, that is aortic regurgitation jet. These are the features, you have AR jet, and MR jet, in a still image of colour Doppler echocardiogram.
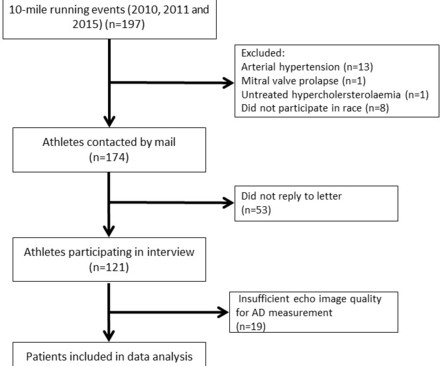
Objective Decreased proximal aortic distensibility (AD) is known to significantly predict all-cause mortality and cardiovascular events among individuals without overt cardiovascular disease. Methods Healthy, normotensive, male Caucasian participants of a 10-mile race were assessed with a 2D echocardiogram and comprehensive interview.
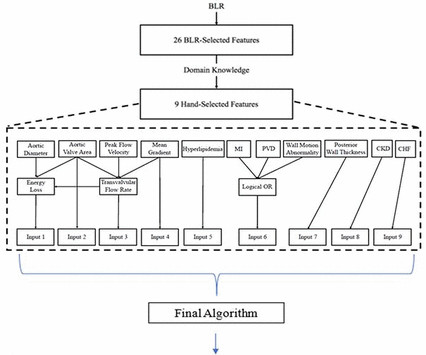
Objective To use echocardiographic and clinical features to develop an explainable clinical risk prediction model in patients with aortic stenosis (AS), including those with low-gradient AS (LGAS), using machine learning (ML). Our algorithm, the Aortic Stenosis Risk (ASteRisk) score, is available online for public use.
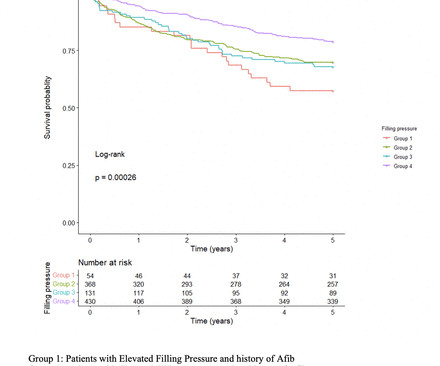
Background Increase in left ventricular filling pressure (FP) and diastolic dysfunction are established consequences of progressive aortic stenosis (AS). However, the impact of elevated FP as detected by pretranscatheter aortic valve replacement (TAVR) echocardiogram on long-term outcomes after TAVR remains unclear.
Background: Symptomatic severe aortic stenosis (AS) remains undertreated with high resultant mortality despite increased growth and availability of aortic valve replacement (AVR) since the advent of transcatheter therapies. The patient cohort had mean age of 7711 years, was 47% female, and had mean aortic valve area 0.80.1
Background:Peak aortic valve Doppler velocity, mean aortic valve gradient, and Doppler estimated aortic valve area are key measures recommended for assessing aortic stenosis severity. Failure to accurately diagnose severe aortic stenosis is critical. Based on the ASE Doppler AVA definition of severe AS (< 1.0
Echocardiogram in parasternal long axis view shows dilated left ventricle, left atrium, aorta and a small portion of the right ventricle, which is usually the outflow region. The large aortic regurgitation jet can be seen as a mosaic jet in the left ventricular outflow tract anterior to the anterior mitral leaflet.
Serial echocardiographic assessments are common in clinical cardiology, e.g., for timing of intervention in mitral and aortic regurgitation. When following patients with serial echocardiograms, each new measur.
Data from the studies demonstrated that AISAP CARDIO enables non-cardiologist physicians to interpret point-of-care echocardiograms just as well as expert cardiologists of the MGB echocardiography lab. James Hillis, MBBS, DPhil, director of Clinical Operations at Mass General Brigham AI.
Unlike the valves on the left side like the mitral and aortic, right sided valves can have some leak. That is, mild mitral regurgitation and mild aortic regurgitation are less common. Mostly, they are detected on highly sensitive tests like echocardiogram. In echocardiogram, the Doppler beam can detect this small leak.
Previous medical interventions included a spectrum of procedures, including catheter-directed thrombectomy for popliteal artery aneurysms with thrombosis, vascular bypass grafting for cerebral-anterior communicating artery aneurysms and arch replacement and stent implantation for aortic dissecting aneurysms.
BackgroundComplex aortic plaque (CAP) is a potential embolic source in patients with cryptogenic stroke (CS). Journal of the American Heart Association, Volume 12, Issue 23 , December 5, 2023.
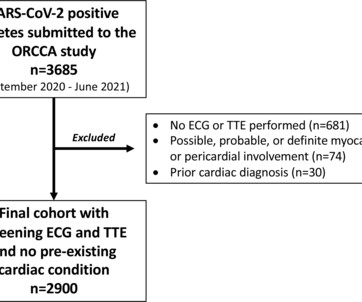
Athletes with an ECG and transthoracic echocardiogram (TTE) and no pre-existing conditions were included. Overall, 6 (0.2%) athletes had major conditions; however, coronary anatomy and aortic dimensions were inconsistently reported and pathology may have been missed.
Similarly, for echocardiogram, what we would do usually is, first we do a clinical history evaluation, then physical examination, and after that only we proceed with echocardiography in our routine work. You can see the two dimensional sector imaging from an echocardiogram and I have marked out the aorta. This could be a conus tissue.
An echocardiogram confirmed aortic stenosis with a large pressure gradient. Now there is much less ST segment deviation, less elevation and less depression. The troponin returned positive, and the maximum troponin was 3.8 The next day, and angiogram showed normal coronary arteries. He awoke and did well.
Residents also received instruction in mitral valve and aortic valve surgery, giving and receiving feedback in the operating room, and the importance of performing ablation. The best parts of the Boot Camp were learning the basics of CT surgery, the vast topics covered (transthoracic echocardiogram, lobectomy, etc.)
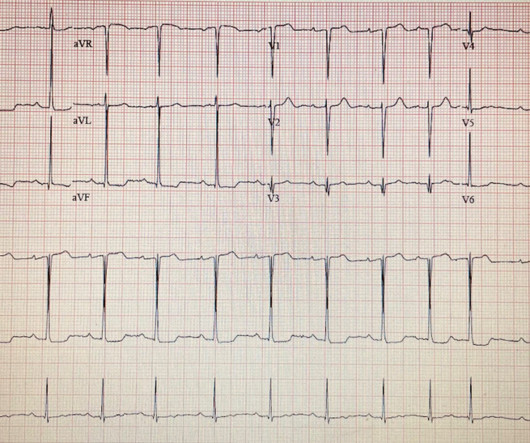
Nossen also pointed out that with voltage this high in the limb leads, you would typically expect some degree of inferior/inferolateral ST depression (the so-called "LVH strain" pattern), and in fact this patient did have severe LVH on subsequent echocardiogram (which Dr. Nossen did not know at the time). The troponin peaked at 25749 ng/L.
The LPA to RPA ratio on initial and most recent echocardiogram, intervention on the LPA at initial surgery and subsequent reintervention on the LPA were compared between the two groups.Results:The 22q11 deletion and control group had a similar mean age at time of study 6.9±3.4 0.27, p=0.002) echocardiogram.
Patent Foramen Ovale 4. Severe calcific Aortic (valve) Stenosis 5. Mechanical prosthetic valve Severe carotid artery stenosis is also implicated in embolic stroke. In the pre-hospital setting the varying modalities needed to rule-in/rule-out these causative factors are not available (eg, Chest X-ray, Echocardiogram, etc).
Another important role is for detection of coronary anomalies, which can also be seen on echocardiogram sometimes. Findings which are sought during an aortogram in tetralogy of Fallot include looking for aortic regurgitation, coronary anomalies, MAPCAs, patent ductus arteriosus and side of the aortic arch.
Echocardiogram is indicated (Correct) C. Start aspirin and Plavix Correct answer: (B) (B) Echocardiogram is indicated. While the first one may radiate to the axilla and base, but usually not into the neck, it does reflect both aortic outflow obstruction and mitral regurgitation in patients with a large gradient.
An echocardiogram showed: Left ventricular hypertrophy concentric. The estimated left ventricular ejection fraction is 58 % Aortic stenosis, mild, 9.0 A third ECG was done about 25 minutes after the first: This shows resolution of all apparent ischemia. The patient thus did not need immediate angiography. mmHg mean gradient.
Transthoracic echocardiogram revealed right to left shunting consistent with a patent foramen ovale (PFO). Further workup with TEE confirmed the presence of a PFO but also detected a mobile echogenic mass on the aortic valve leaflet, indicative of papillary fibroelastoma (PFE).
Look at the aortic outflow tract. The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Aortic angiogram did not reveal aortic dissection. In fact, bedside ultrasound might even find severe aortic stenosis. What do you see?
The next morning the patient went for his routine echocardiogram, where the operator noticed a dilated aortic root at 5.47 cm with severe aortic insufficiency. The team was notified and they ordered a stat aortagram which showed type A aortic dissection from the aortic valve to the iliacs.
The image shown here is an animated 2 dimensional echocardiogram. This one is an older mode known as time-motion mode or M-Mode echocardiogram. Opening and closing movements of the aortic and mitral valves are visible. The image shows the blue coloured descending aortic flow on colour Doppler.
Hopefully a repeat echocardiogram will be performed outpatient. Systolic function normal by visual assessment only, unable to visualize well for further characterization. 1900: RBBB and LAFB are almost fully resolved. 2300: QRS now within normal limits. No other significant injuries were found. The patient did well and was discharged.
They also wanted an aortic CT which was negative. First troponin I returns at 48 ng/L ECG 5 143 min No significant change ECG 6 261 min Same hs Troponin I profile (peaked at 1849): Formal Echocardiogram SUMMARY The estimated left ventricular ejection fraction is 74 %. This is a "Transient OMI". Eur Heart J 2018. Full text link.
Blunt cardiac injury my result in : 1) Acute myocardial rupture with tamponade 2) Valve rupture (tricuspid, aortic, mitral) 3) Coronary thrombosis or dissection (and thus Acute MI) from direct coronary blunt injury 4) Dysrhythmias of all kinds. She was discharged to home feeling just fine.
The echocardiogram showed a normal EF without any abnormalities. With ongoing transcutaneous pacing, Cardiology emergently took the patient to the cath lab for temporary pacing wire placement via right IJ which she tolerated well. Troponins were all negative. There was no apparent reversible cause found for the worsening heart block.
He visited an outpatient clinic for it and an echocardiogram and exercise stress test was normal. As his pain was very severe, emergency physicians concerned of aortic dissection and ordered a thoracic CT scan. He has 40 packs-year of smoking history. There was no premature cardiovascular diseases or sudden death in his family.
Category 2 : An increase in myocardial oxygen demand due to tachycardia, elevated ventricular afterload (BP or aortic stenosis), or increased wall stretch (admittedly this latter is more complicated) or a decrease in oxygen supply due to hypotension, anemia, hypoxia, or a combination of all of the above. Aortic Stenosis f.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content