This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Getty Images milla1cf Wed, 06/05/2024 - 20:33 June 5, 2024 — Edwards Lifesciences announced it has entered into a definitive agreement to sell its CriticalCare product group to BD (Becton, Dickinson and Company), in an all-cash transaction valued at $4.2
Edwards Lifesciences is going all-in on structural heart and heart failure, acquiring aortic valve-maker JenaValve Technology and implantable heart failure monitor company Endotronix for $1.2B The post Edwards Acquires JenaValve and Endotronix, Expands into Aortic Regurgitation and Heart Failure appeared first on Cardiac Wire.
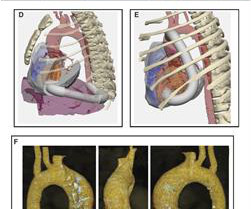
With this longer lifespan, calcific aortic stenosis (AS) was identified as an emerging critical risk factor for cardiac death in older patients. Intervention to relieve critical AS has the potential for immediate improvement in healthspan and lifespan. years by 4.3 years (30%).
The software generates accurate reports in minutes using inexpensive devices, enabling emergency medicine, criticalcare, internal medicine, hospitalists and primary care physicians to make informed care decisions at the bedside.
ET – E/M, CriticalCare Q&A 10:45 a.m. Summarize the necessary documentation and regulations relevant to criticalcare and cardiothoracic surgery E/M services for 2023. ET – Adult Cardiac Q&A 5:15 p.m. ET – 6:00 p.m. ET – Congenital Cardiac Q&A 6:00 p.m. ET – 6:45 p.m. ET – 10:45 a.m. ET – 11:30 a.m.
They also wanted an aortic CT which was negative. Then the patient's pain then resolved spontaneously after 2 sublingual nitroglycerine and another ECG was recorded ECG 2 at 16 minutes ST ELEVATION CONSISTENT WITH INJURY, PERICARDITIS, OR EARLY REPOLARIZATION Overread same Smith : The T-waves are now MUCH smaller. This is a "Transient OMI".
There was high suspicion of OMI, so patient was brought to criticalcare area and another ECG was recorded just 7 minutes later as the pain had diminished to 4/10. Due to the severity of the pain and the high BP, they obtained an aortic dissection CT. especially since this Chest CT was done to rule out aortic dissection ).
Adult Cardiac Surgery Database Lead Author Title Publication Date Jacob Raphael Red Blood Cell Transfusion and Pulmonary Complications: The Society of Thoracic Surgeons Adult Cardiac Surgery Database Analysis The Annals of Thoracic Surgery January 2024 Joseph Sabik Multi-Arterial versus Single-Arterial Coronary Surgery: Ten Year Follow-up of One Million (..)
Program Designations Access and Publications (A&P) 1 Participant User File (PUF) 2 Task Force on Funded Research (TFR) 3 Special Projects 4 Adult Cardiac Surgery Database Lead Author Title Publication Date William Keeling 2 National Trends in Emergency Coronary Artery Bypass Grafting European Journal of Cardiothoracic Surgery October 2023 Jake (..)
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the criticalcare area and the cath lab was activated. The blood pressure was 170/100 in the criticalcare area. Important: It is exceedingly rare for an anterior STEMI to be due to Aortic Dissection. Her initial BP was 203/124.
There was some question of whether the patient was having abdominal pathology, and she also had a history of aortic pathology, so a chest abd/pelvic with aorta angiogram was ordered. There is STE in V5-6. There are new Q-waves in aVL, V5-6. If this were ACUTE (vs. SUBACUTE) OMI, that would result in an undesirable delay.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content