This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Compared to the survival group, those in the mortality group exhibited significantly higher rates of exploratory thoracotomy, intra-aortic balloon pump usage, extracorporeal membrane oxygenation application, gastrointestinal bleeding incidents, and acute renal failure occurrences.
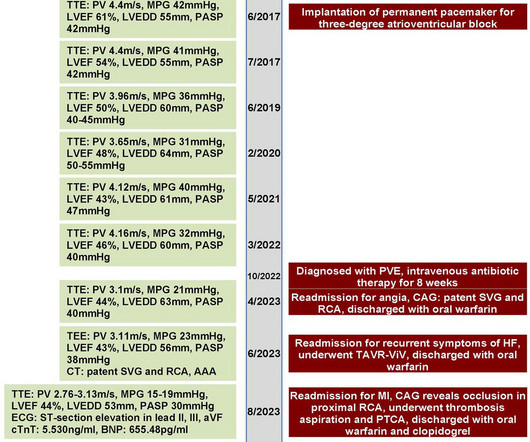
A 70-year-old female patient with a history of bioprosthetic aortic valve replacement and coronaryarterybypassgraft presented with bioprosthetic valve failure secondary to prosthetic valve endocarditis. This resulted in early death due to myocardial infarction and acute heart failure.
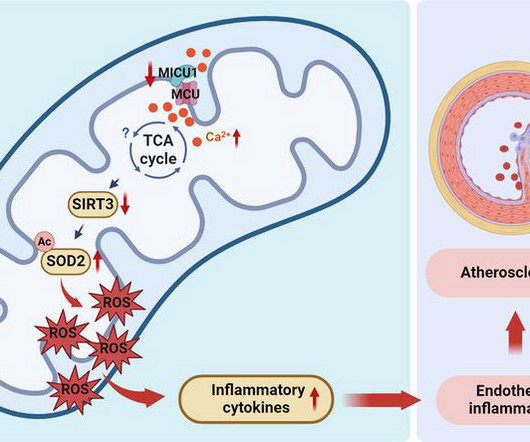
Of clinical relevance, we observed decreased MICU1 expression in the endothelial layer covering human atherosclerotic plaques and in human aortic endothelial cells exposed to serum from patients with coronaryartery diseases (CAD).
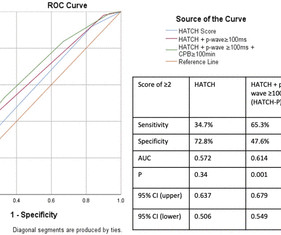
Background Atrial fibrillation (AF) following coronaryarterybypassgraft surgery (CABG) is common and results in significant increases in hospital stay and financial encumbrance. Objective Determine and use the predictors of postoperative AF (POAF) following CABG to develop a new predictive screening tool. ±33.9
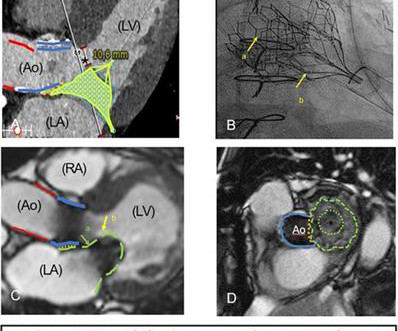
Pre-operative coronary angiography and concomitant, planned coronaryarterybypass are infrequently performed with type A aortic dissection repair. We present a case in which pre-operative coronary computed to.
Objective To investigate the impact of prior coronaryarterybypassgrafting (CABG) and coronary lesion complexity on transcatheter aortic valve replacement (TAVR) outcomes for aortic stenosis. The median CABG SYNTAX score was 16 (interquartile range: 9.0–23),
End-Stage Renal Disease (ESRD) is an independent risk factor in outcomes for traditional coronaryarterybypassgrafting (TRAD-CAB) utilizing aortic cross-clamping and cardioplegic arrest. In order to determin.
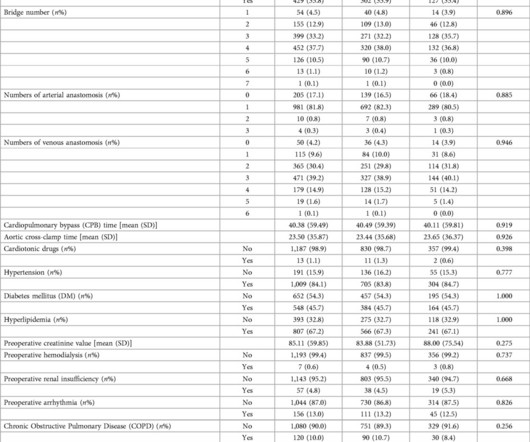
Subsequently, LASSO model was used to identify 11 important features, which were mechanical ventilation time, preoperative creatinine value, preoperative renal insufficiency, diabetes, the use of an intra-aortic balloon pump (IABP), age, Cardiopulmonary bypass time, Aortic cross-clamp time, Chronic Obstructive Pulmonary Disease (COPD) history, preoperative (..)
Penetrating aortic ulcer (PAU) represents a subset of acute aortic syndromes characterized by high rupture risk and management challenges, particularly in elderly patients with significant comorbidities.
The goal of the TCW trial was to test the noninferiority and, if positive, superiority, of percutaneous coronary intervention (PCI) with transcatheter aortic valve implantation (TAVI) compared with surgical aortic valve replacement (SAVR) and coronaryarterybypassgrafting (CABG) in severe aortic stenosis (AS) with comorbid coronaryartery disease (..)
We estimate the relationship between local deprivation ranking and differences in volumes of aortic valve replacement, which include transcatheter aortic valve replacement (TAVR) and surgical aortic valve replacement (SAVR), versus coronaryarterybypassgraft surgery and laparoscopic colectomy (LC).
Background Redo sternotomy aortic root surgery is technically demanding, and the evidence on outcomes is mostly from retrospective, small sample, single-centre studies. We report the trend, early clinical results and outcome predictors of redo aortic root replacement over 20 years in the United Kingdom. Emergency surgery (OR: 3.95, 2.27–6.86,
The academic medical centers received three-star ratings in isolated coronaryarterybypassgrafting (CABG) and isolated mitral valve replacement and repair (MVRR) surgeries. Jersey Shore University Medical Center also received a three-star rating in isolated aortic valve replacement (AVR) surgery.
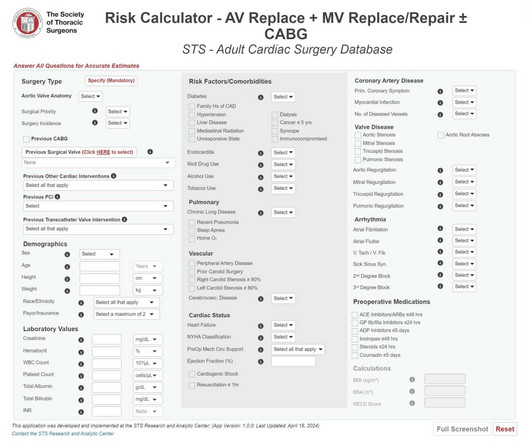
SAVR after TAVR Surgical aortic valve replacement after prior TAVR is the fastest-growing cardiac surgery procedure in the U.S. The STS rolled out all three interactive, mobile-friendly risk calculators in April 2024, adding to its existing portfolio of risk calculators for adult cardiac surgery.
BackgroundLp(a) (lipoprotein(a)) is an independent risk factor for calcific aortic valve stenosis (CAVS). Journal of the American Heart Association, Ahead of Print. Whether patients with CAVS and high Lp(a) levels are at higher risk of valvular or cardiovascular events is unknown. The maximal followup time was set to 5 years.
There were no significant differences between the two groups regarding CPB time, aortic cross-clamp time, duration of mechanical ventilation and length of stay in ICU (p<0.05). However, the incidence of POD was significantly lower in the intervention group compared with the control group (22.25% vs 42.2%, p=0.035).
It uses a three-star scale (3=better than expected, 2=as expected, 1=worse than expected) to rate institutions across five common cardiovascular procedures: coronaryarterybypassgrafting (CABG); aortic valve replacement (AVR); AVR and CABG; mitral valve replacement/repair (MVRR); and MVRR and CABG.
STS leveraged contemporary national data from the STS Adult Cardiac Surgery Database between July 2017 and December 2023 to analyze outcomes of 32,938 patients that underwent multi-valve surgery involving replacement of the aortic valve, plus replacement or repair of the mitral valve, with and without concomitant coronaryarterybypassgrafting.
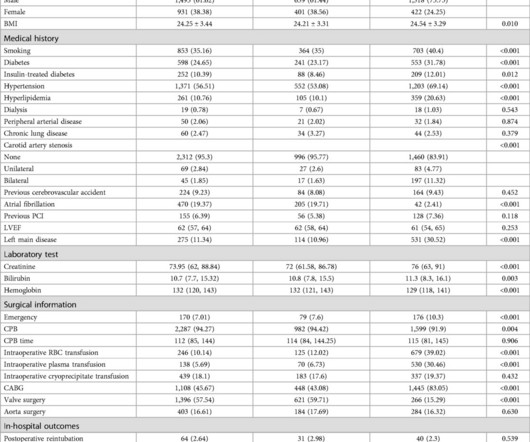
Predictive variables were selected based on clinical expertise and prior literature, and a nomogram was developed using LASSO regression and multiple logistic regression.
Prior transapical transcatheter aortic valve replacement (TA-TAVR) may complicate the procedure and is therefore considered a relative contraindication. He had already undergone cardiac surgery in the form of coronaryarterybypassgrafting at the age of 64 and TA-TAVR at 79 years.
Introduction The presence of non-coronary atherosclerosis (NCA) in patients with coronaryartery disease is associated with a poor prognosis. We have studied whether NCA is also a predictor of poorer outcomes in patients undergoing coronaryarterybypassgrafting (CABG).
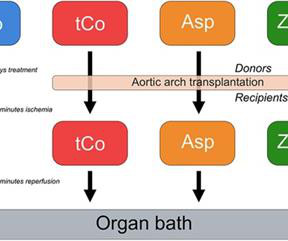
Introduction Coronaryarterybypassgrafting (CABG) is the most common cardiac surgical procedure. The prognosis of revascularization via CABG is determined by the patency of the used grafts, for which an intact endothelium is essential. There was also a non-ischemia-reperfusion control group ( n = 8).
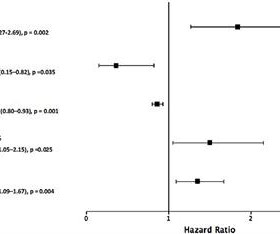
per year) and concomitant coronaryarterybypassgrafting versus isolated valve surgery (HR 0.58, 95% CI 0.35 to 4.01) and aortic valve disease versus mitral valve disease (HR 2.16, 95% CI 1.20 Increasing age (HR 0.97, 95% CI 0.95 Being a man (HR 2.30, 95% CI 1.32
Concomitant procedures performed were LAA ligation in 20 (69.0%), aortic valve replacement in 5 (17.2%), and coronaryarterybypassgrafting in 3 (10.3%) patients. Peak left ventricular outflow tract (LVOT) gradients were 40.5 ± 34.9 mmHg mmHg at rest and 56.5 ± 34.9 mmHg mmHg after provocation.
It is commonly used for various cardiac and thoracic procedures , including but not limited to coronaryarterybypassgrafting (CABG), mitral valve repair or replacement, and lung surgeries. Incision Placement One of the primary distinctions of minithoracotomy is the location of the incision.
Since the clip is inserted through an artery, it eliminates the need for risky chest incisions. Aortic Valve Replacement (AVR): AVR is a minimally invasive procedure in which the surgeon makes a small incision and allows the heart to continue to beat during the entire procedure. Then, they place a graft.
Look at the aortic outflow tract. The diagnostic coronary angiogram identified only minimal coronaryartery disease, but there was a severely calcified, ‘immobile’ aortic valve. Aortic angiogram did not reveal aortic dissection. What do you see? Answer below in the still shot.
Removing these barriers would allow surgeons, physicians, hospitals, health systems, and others to conduct longitudinal analyses and gain new insights into long-term outcomes for patients undergoing procedures such as coronaryarterybypassgrafting (CABG)—the most common operation performed by cardiac surgeons.
Adult Cardiac Surgery Database Lead Author Title Publication Date Jacob Raphael Red Blood Cell Transfusion and Pulmonary Complications: The Society of Thoracic Surgeons Adult Cardiac Surgery Database Analysis The Annals of Thoracic Surgery January 2024 Joseph Sabik Multi-Arterial versus Single-ArterialCoronary Surgery: Ten Year Follow-up of One Million (..)
Program Designations Access and Publications (A&P) 1 Participant User File (PUF) 2 Task Force on Funded Research (TFR) 3 Special Projects 4 Adult Cardiac Surgery Database Lead Author Title Publication Date William Keeling 2 National Trends in Emergency CoronaryArteryBypassGrafting European Journal of Cardiothoracic Surgery October 2023 Jake (..)
We hypothesize the presence of comorbid cardiac disease has a synergistic effect on cognitive impairment in patients with asymptomatic CAS.Methods:Patients with 80% internal carotid artery stenosis with no history of stroke were recruited from inpatient and outpatient practices at a single, large, comprehensive stroke center.
Compared with OPCABG, generalized HCR was associated with a signicantly lower intra-aortic balloon pump (IABP) implantation rate (2.7% The residual SYNTAX score was similar between two groups (6.35.5 for generalized HCR vs. 6.85.3 for OPCABG; P=0.486). vs. 9.9%; P=0.027) and shorter postoperative length of stay (6.33.2 vs. 7.73.0;
TTFM demonstrated superior flow rates in artery-on-vein grafts [50 (4070) ml/min] compared to vein-on-vein grafts [40 (3053.5), p<0.001].ConclusionsWhen Intraoperative TTFM showed excellent flow rates, especially when arterialgrafts were used.
More troponin values were measured at the cardiac center: 2327- 267 ng/L 0821- 355 ng/L 1108- 305 ng/L An echocardiogram on day three of the patients admission showed an ejection fraction of 46% with abnormal basal inferior and basal lateral segments, and severe aortic stenosis. What "initiates" the aortic stenosis cascade?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content