This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Submitted and written by Quinton Nannet, MD, peer reviewed by Meyers, Grauer, Smith A woman in her 70s recently diagnosed with COVID was brought in by EMS after she experienced acute onset sharp midsternal chestpain without radiation or dyspnea. She was taken immediately for a CT angiogram of the chest, abdomen and pelvis.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chestpain. Several hours prior to presentation, while driving his truck, he started experiencing new central chestpain, without radiation, aggravating/alleviating factors, or other associated symptoms.
Description of Case:A 64-year-old male with complex medical history, including infective endocarditis of the aortic valve requiring surgical replacement with a bioprosthetic valve and recurrent infective endocarditis of the bioprosthetic valve, presented with two hours of crushing chestpain and found to have ST elevations.
If you saw this ECG only knowing that it is an acute chestpain patient, what would be your interpretation? However, in the context of the first ECG and the waning chestpain, this is diagnostic of reperfusion. Due to the severity of the pain and the high BP, they obtained an aortic dissection CT.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. Smith comment: This patient did not have a bedside ultrasound. Look at the aortic outflow tract. Aortic angiogram did not reveal aortic dissection.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. Left main? 3-vessel disease?
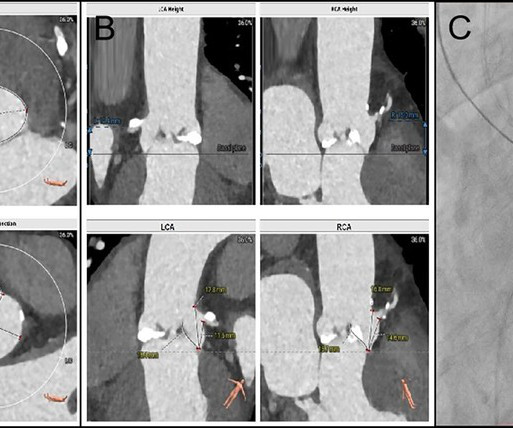
BackgroundFollowing transcatheter aortic valve replacement, acute coronary obstruction is infrequent but potentially life-threatening, while delayed coronary obstruction is even more uncommon.Case summaryA 69-year-old male underwent TAVR and subsequently developed an acute obstruction in the left main coronary artery.
No prior exertional complaints of chestpain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. I sent this ECG to Dr. Smith, with the only information that it is a 17 year old with chestpain. 24 yo woman with chestpain: Is this STEMI?
Most cases go undiagnosed until the condition advances enough to create symptoms such as shortness of breath, chestpain or fatigue. AI algorithms could further improve care by using data from ultrasounds and other imaging devices to develop a digital twin of each patient.
A man in his 60's presented after 4 days of chestpain, with some increase of pain on the day of presentation. Exact pain history was difficult to ascertain. An intra-aortic balloon pump was placed, and the patient was taken for immediate surgical repair but did not survive. There was some SOB. How acute is it?
An elderly patient with a ruptured abdominal aortic aneurysm: Formal ECG Interpretation (final read in the chart!) : "Inferior ST elevation, lead III, with reciprocal ST depression in aVL." Case 3 : Male in 30's with chestpain, cough, and fever. A bedside ultrasound was done by the emergency physician, using Speckle Tracking.
Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope).
Case 1: 20-something woman with chestpain Case 2: 50-something man with chestpain Case 1 A 20-something yo woman presented in the middle of the night with severe crushing chestpain. Important: It is exceedingly rare for an anterior STEMI to be due to Aortic Dissection. Case 2 A 50-something y.o.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content