This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Until now, patients with aorticstenosis—a narrowing of one of the heart's main valves—have had to wait until symptoms become severe before undergoing valve replacement.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. It was not relieved by anything. He had no previous medical history.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chestpain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
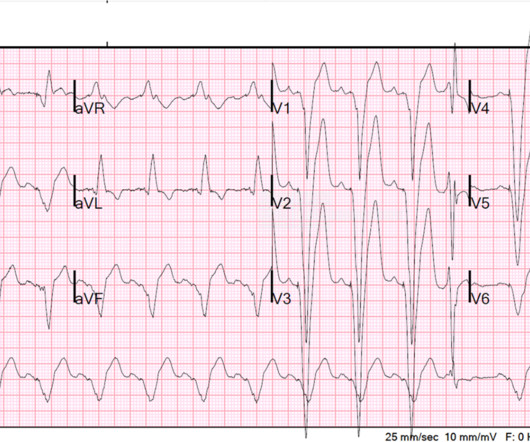
There was no chestpain. V1 and V2 are probably placed too high on the chest given close morphological similarity to aVR. The LM has an irregular 30% distal stenosis, followed by an 80% ostial LAD stenosis, and total occlusion of the LAD proximally with TIMI grade 1 flow in the distal vessel. Type II ischemia.
If you’ve been diagnosed with aorticstenosis, you might have come across the term TAVR. Understanding AorticStenosis The aortic valve regulates blood flow from your heart’s main pumping chamber to the rest of your body. In aorticstenosis, the valve leaflets stiffen and narrow, restricting blood flow.
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. They also wanted an aortic CT which was negative. Wellen's waves indicate that, when the patient was having chestpain, there was occlusion. What do you think the prehospital ECG showed (with pain)?
He presented with chestpain, not relieved by nitro, pain reproducible on exam and centered around the pacemaker insertion site. Here is his ECG one month prior, on admission for chestpain at that time also: Similar ratios. LV Ejection Fraction at the time of this hospitalization was 10%.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chestpain. Several hours prior to presentation, while driving his truck, he started experiencing new central chestpain, without radiation, aggravating/alleviating factors, or other associated symptoms.
If you saw this ECG only knowing that it is an acute chestpain patient, what would be your interpretation? However, in the context of the first ECG and the waning chestpain, this is diagnostic of reperfusion. Due to the severity of the pain and the high BP, they obtained an aortic dissection CT.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. Look at the aortic outflow tract. Aortic angiogram did not reveal aortic dissection. What do you see? Answer below in the still shot.
But the symptoms returned with similar pattern – provoked by exertion, and alleviated with rest; except that on each occasion the chestpain was a little more intense, and the needed recovery period was longer in duration. AorticStenosis f. Left Main stenosis (not thrombosed) c. This results in Type I MI.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. 2 cases of AorticStenosis: Diffuse Subendocardial Ischemia on the ECG. Anything more on history?
60-something with h/o MI and stents presented with chestpain radiating to the back and nausea/vomiting. There was concern for aortic dissection, so a CT was done and was negative. Time zero What do you think? There is inferior ST elevation. Is it normal variant? Is it ischemic (OMI)? Pericarditis?
There is ventricular hypertrophy in the absence of abnormal loading conditions, such as aorticstenosis, or hypertension, for example – of which the most common variant is Asymmetric Septal Hypertrophy. As a brief review, HCM is a genetically inherited disorder that produces structural disarray in the myocardial cells.
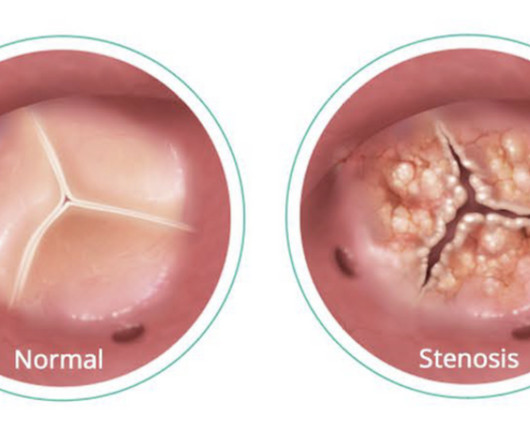
Aorticstenosis is a narrowing of the aortic valve which prevents the aortic leaflets from opening and closing properly. Patients with aorticstenosis often have heart murmurs and experience debilitating symptoms including chestpain, dizziness, fatigue, shortness of breath and an irregular heartbeat.
The Most Common Form of HVD One of the most prevalent and serious forms of heart valve disease is aorticstenosis (AS), a condition characterized by the narrowing of the aortic valve opening, which affects approximately 5% of adults over 65a number expected to more than double by 2050.
Aorticstenosis is a narrowing of the aortic valve which prevents the aortic leaflets from opening and closing properly. Patients with aorticstenosis often have heart murmurs and experience debilitating symptoms including chestpain, dizziness, fatigue, shortness of breath and an irregular heartbeat.
1, 2024 — Researchers at UTHealth Houston have identified genetic variants linked to a rare form of bicuspid aortic valve disease that affects young adults and can lead to dangerous and potentially life-threatening aortic complications. tim.hodson Wed, 09/04/2024 - 15:53 Sept.
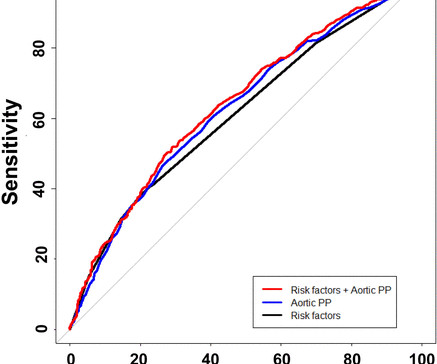
We aimed to determine whether invasive aortic PP is associated with coronary microvascular endothelial dysfunction (CMED) and/or coronary microvascular endothelial independent dysfunction (CMEID) in patients with non-obstructed CAD. The patients were classified based on whether aortic PP was high (≥50 mm Hg). to 1.78; p=0.003).
Most cases go undiagnosed until the condition advances enough to create symptoms such as shortness of breath, chestpain or fatigue. Valvular heart disease, a condition in which any of the heart’s four valves are damaged or diseased, afflicts 2.5 percent of all Americans and 13 percent of Americans over age 80.
Noel Bairey Merz, MD , director of the Barbra Streisand Women's Heart Center , will participate in a cardiovascular health for women session, “Where Are We Now: From WISE to CHESTPAIN Guidelines,” Sunday, April 7, 12:45-12:52 p.m. Natalie Bello, MD, MPH , director of Hypertension Research, will present “What’s Sex Got to Do With It?
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The history in today's case with sudden loss of consciousness followed by chestpain is very suggestive of ACS and type I ischemia as the cause of the ECG changes. What do you think?
It showed reduced LV function — significant concentric LVH — a dilated left atrium — severe aorticstenosis ( seemingly in need of prompt valve replacement ) — and at least moderate pulmonary hypertension , with resultant moderate pulmonary regurgitation. The plan was to proceed as soon as possible with aortic valve replacement.
He has never had any chestpain. While the first one may radiate to the axilla and base, but usually not into the neck, it does reflect both aortic outflow obstruction and mitral regurgitation in patients with a large gradient. He has no known prior medical history and does not take any medications.
An elderly patient with a ruptured abdominal aortic aneurysm: Formal ECG Interpretation (final read in the chart!) : "Inferior ST elevation, lead III, with reciprocal ST depression in aVL." Case 3 : Male in 30's with chestpain, cough, and fever. What do you think? Does he need a stress test? --Is
His comments/questions are inserted below the ECG: A 50-something woman presented with 3 days of intermittent chestpain that became worse on the day of presentation, with diaphoresis and radiation to the left arm, as well as abdominal pain. TIMI 0/1 flow).(61,62) Knotts et al.
Aortic Dissection, Valvular (especially AorticStenosis), Tamponade. Check : [vitals, SOB, ChestPain, Ultrasound] If the patient has Abdominal Pain, ChestPain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope).
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
This was submitted by a paramedic, Hailey Kennedy A late 50s male called 911 following 2 hours of chestpain that started while working at his desk. He reported the crushing chestpain radiated down his left arm. He presented to the ED for evaluation chestpain. Pain was improved but not gone upon arrival.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content