This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
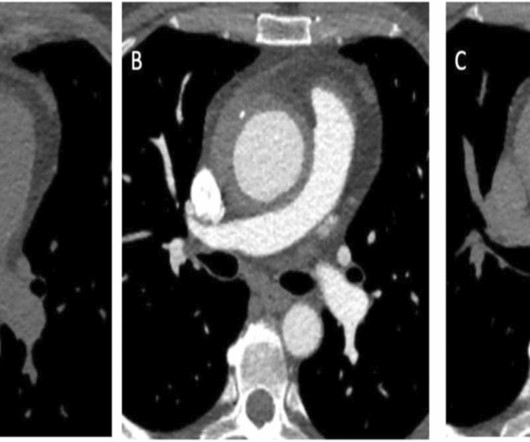
Written by Willy Frick A 67 year old man with a history of hypertension presented with three days of chestpain radiating to his back. Due to the chestpain radiating into the patient's back, the ER physician ordered CTA chest to rule out aortic dissection. He had associated nausea, vomiting, and dyspnea.
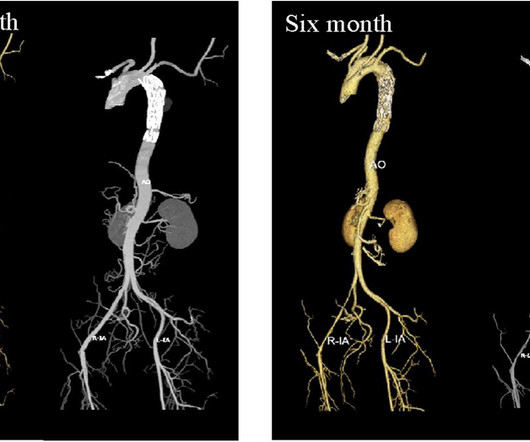
BackgroundDouble aortic arch (DAA) with type B aortic dissection in adults is a rare aortic vascular disease. Computed tomography angiography (CTA) indicated a double aortic arch anomaly with localized dissection of the descending aorta.
Written by Willy Frick A man in his early 40s with BMI 36, hypertension, and a 30 pack-year smoking history presented with three days of chestpain. He described it as a mild intensity, nagging pain on the right side of his chest with nausea and dyspnea. It started while he was at rest after finishing a workout.
Though a rare condition, acute type A aortic dissection (ATAAD) is associated with high morbidity and mortality; hence, timely diagnosis and surgery are important to reduce the risk of mortality. If the dissection extends into the aortic arch branches, ensuring adequate cerebral perfusion during surgery is crucial to preventing stroke.
Until now, patients with aortic stenosis—a narrowing of one of the heart's main valves—have had to wait until symptoms become severe before undergoing valve replacement.
Clinical introduction A man in his 40s with a history of hyperlipidaemia presented with intermittent, dull left-sided chestpain for 2 weeks that was not consistently exertional. Physical examination, an ECG, basic laboratories and a chest X-ray were unremarkable. He did not smoke or use alcohol or illicit drugs.
It is not always possible to be certain about the origin of chestpain just by its characteristics as the variation between individuals is quite a bit. A medical opinion should be sought in case of any significant chestpain so that important ailment is not missed. A pain lasting more than 30 minutes is usual.
This is another case written by Pendell Meyers (who is helping to edit the blog and has many great recent posts) Case A 45 year old man was driving to work when he experienced acute onset sharp left sided chestpain with paresthesias of the left arm. A repeat ECG was recorded with pain 2/10: Not much change.
After 24 hours, the patient was readmitted to the hospital with chestpain and troponin elevation, without ECG changes. A transthoracic echocardiogram (TTE) revealed a mobile mass on the right coronary cusp of the aortic valve ( figure 1 , ). Figure 1 A mobile mass (1.88
In this ECG Cases blog we look at 10 cases of patients with chestpain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
A middle aged male presented at midnight after 14 hours of constant, severe substernal chestpain, radiating to his throat and to bilateral jaws, and associated with diaphoresis. The pain was not positional, pleuritic, or reproducible. It was not relieved by anything. He had no previous medical history.
An elderly woman presented with chestpain that radiated to the back for several hours. The first troponin returned at 0.099 ng/mL (elevated, consistent with Non-Occlusion MI) Providers were concerned with aortic dissection, so they order a chest aorta CT. It is essentially normal.
Submitted and written by Quinton Nannet, MD, peer reviewed by Meyers, Grauer, Smith A woman in her 70s recently diagnosed with COVID was brought in by EMS after she experienced acute onset sharp midsternal chestpain without radiation or dyspnea. She was taken immediately for a CT angiogram of the chest, abdomen and pelvis.
Submitted by Ali Khan MD and James Mantas MD, MS, written by Pendell Meyers A man in his 50s with history of diabetes, hypertension, and tobacco use presented to the ED with 24 hours of worsening left sided chestpain radiating to the back, characterized as squeezing and pinching, associated with shortness of breath.
Post op chestpain Typical of post-op pericarditis (postpericardiotomy syndrome) There is ST Elevation in II > III, and STE in V3-5, but with flat T-wave. Angiogram: Severe 95% hazy distal LM Severe 80% ostial LAD, 100% occluded distal LAD thought to be due to distal embolization from the lesion in the proximal LAD.
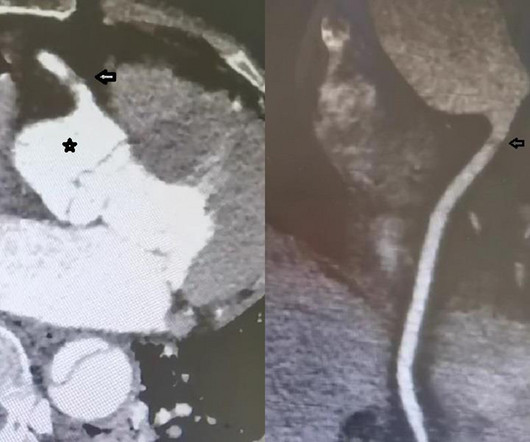
Background Type A aortic dissection (TAAD) with coronary involvement is rare but potentially fatal. Case presentation Here, we describe a 52-year-old woman who presented with sudden chestpain. Proper myocardial protection during surgery is essential. CT angiography revealed TAAD with right coronary artery involvement.
Left ventricular afterload reduction is essential to decrease the trans-se ptal pressure gradient and thus decrease shunt volume, making a larger proportion of the blood flow from the left ventricle through the aortic valve. Not all patients with acute ( or recent ) MI have chestpain with their event.
A 54-year-old female presented with recurrent abdominal pain and new onset chestpain. Chest computed-tomography angiogram detected a thoracic aortic aneurysm with suspected Type A intramural hematoma (IMH) versu.
The provider had sent the patient for an aortic dissection scan which had shown extremely heavy calcification of the LAD. The patient had continued to have chestpain.
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. They also wanted an aortic CT which was negative. Wellen's waves indicate that, when the patient was having chestpain, there was occlusion. What do you think the prehospital ECG showed (with pain)?
If you’ve been diagnosed with aortic stenosis, you might have come across the term TAVR. Understanding Aortic Stenosis The aortic valve regulates blood flow from your heart’s main pumping chamber to the rest of your body. In aortic stenosis, the valve leaflets stiffen and narrow, restricting blood flow.
The patient reported no chestpain or shortness of breath. Cystic formation of the foramen ovale Aortic sinus aneurysm Left. Clinical introduction A woman is her 60s with no medical history presented to the hospital with palpitations and occasional nausea. Observations revealed a normal temperature of 36.5°C
Context: a man in his 40s presented to the emergency department with 1 day of sudden onset chestpain. Two weeks ago he had a significant MVC with many severe injuries, including aortic injury s/p endovascular repair. Smith responded: "Not OMI. Pericarditis maybe."
Previous medical interventions included a spectrum of procedures, including catheter-directed thrombectomy for popliteal artery aneurysms with thrombosis, vascular bypass grafting for cerebral-anterior communicating artery aneurysms and arch replacement and stent implantation for aortic dissecting aneurysms.
He presented with chestpain, not relieved by nitro, pain reproducible on exam and centered around the pacemaker insertion site. Here is his ECG one month prior, on admission for chestpain at that time also: Similar ratios. LV Ejection Fraction at the time of this hospitalization was 10%.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chestpain. Several hours prior to presentation, while driving his truck, he started experiencing new central chestpain, without radiation, aggravating/alleviating factors, or other associated symptoms.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
There was no chestpain. V1 and V2 are probably placed too high on the chest given close morphological similarity to aVR. The fall was not a mechanical etiology. He denied any specific prodrome of gross palpitations, however did endorse feeling quite dizzy just before the event. Type II ischemia.
If you saw this ECG only knowing that it is an acute chestpain patient, what would be your interpretation? However, in the context of the first ECG and the waning chestpain, this is diagnostic of reperfusion. Due to the severity of the pain and the high BP, they obtained an aortic dissection CT.
Description of Case:A 64-year-old male with complex medical history, including infective endocarditis of the aortic valve requiring surgical replacement with a bioprosthetic valve and recurrent infective endocarditis of the bioprosthetic valve, presented with two hours of crushing chestpain and found to have ST elevations.
A 40-something woman presented to the ED having had “heartburn” overnight and then worsening chestpain 1 hour prior to arrival. Case continued The patient continued having pain. The patient arrived looking like an aortic dissection patient, so CTA was done and negative." The patient looked ill.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
Another important serious disease which has to be thought of in a person with pain in the chest or upper back is aortic dissection. Aortic dissection is tear in the inner lining of the aorta. Blood seeps into the wall of the aorta and spreads along the wall of the aorta.
A 79‐year‐old man with a strong family history of arterial dissection, hypertension, coronary artery disease, and obesity experienced intense chestpain and left hemiparesis secondary to Type A aortic dissection with extension from the innominate artery to the right carotid bifurcation.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. Look at the aortic outflow tract. Aortic angiogram did not reveal aortic dissection. What do you see? Answer below in the still shot.
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chestpain.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. Left main? 3-vessel disease?
60-something with h/o MI and stents presented with chestpain radiating to the back and nausea/vomiting. There was concern for aortic dissection, so a CT was done and was negative. Time zero What do you think? There is inferior ST elevation. Is it normal variant? Is it ischemic (OMI)? Pericarditis?
But the symptoms returned with similar pattern – provoked by exertion, and alleviated with rest; except that on each occasion the chestpain was a little more intense, and the needed recovery period was longer in duration. Aortic Stenosis f. Aortic Stenosis [No Hx syncope, and no systolic murmur] f. Severe Hypoxia b.
There is ventricular hypertrophy in the absence of abnormal loading conditions, such as aortic stenosis, or hypertension, for example – of which the most common variant is Asymmetric Septal Hypertrophy. As a brief review, HCM is a genetically inherited disorder that produces structural disarray in the myocardial cells.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
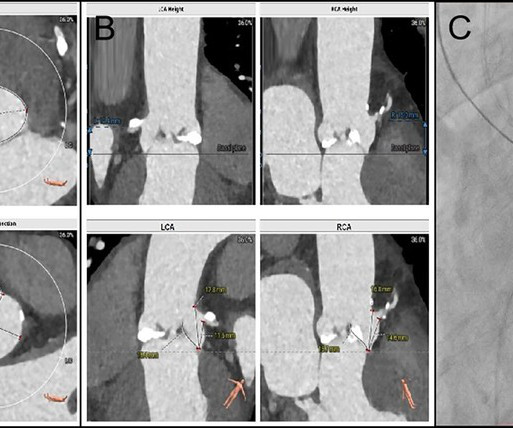
BackgroundFollowing transcatheter aortic valve replacement, acute coronary obstruction is infrequent but potentially life-threatening, while delayed coronary obstruction is even more uncommon.Case summaryA 69-year-old male underwent TAVR and subsequently developed an acute obstruction in the left main coronary artery.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content