This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
ST depression is common BOTH after resuscitation from cardiacarrest and during atrial fib with RVR. Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiacarrest, after defibrillation, and after cardioversion. The patient was cardioverted. This was done.
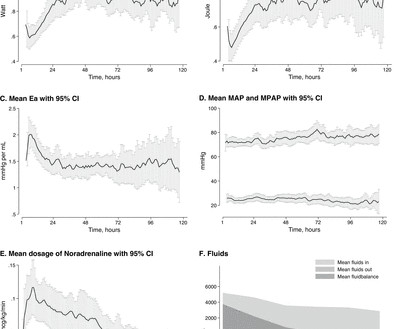
Background Circulatory failure after out-of-hospital cardiacarrest (OHCA) as part of the postcardiac arrest syndrome (PCAS) is believed to be caused by an initial myocardial depression that later subsides into a superimposed vasodilatation.
(MedPage Today) -- Not all defibrillator pad positions may work equally well for patients with shockable out-of-hospital cardiacarrest. JAMA Network Open) Medical therapy for aortic stenosis? Early clinical data on evogliptin were disappointing.
An echocardiogram confirmed aortic stenosis with a large pressure gradient. Now there is much less ST segment deviation, less elevation and less depression. The troponin returned positive, and the maximum troponin was 3.8 The next day, and angiogram showed normal coronary arteries. He awoke and did well.
Patients with significant pulmonary oedema or aortic valve (AV) closure during venoarterial extracorporeal membrane oxygenation (VA-ECMO) were randomized to early left ventricular (LV) unloading or conventional strategy groups (1:1). The primary endpoint was the rate of weaning from VA-ECMO during index admission.
This patient is actively dying from a left main coronary artery OMI and cardiacarrest from VT/VF or PEA is imminent! Complete LMCA occlusion is associated with clinical shock and/or cardiacarrest. The arterial blood gas showed a lactic acidosis with a lactate level of 17mmol/L.
It showed reduced LV function — significant concentric LVH — a dilated left atrium — severe aortic stenosis ( seemingly in need of prompt valve replacement ) — and at least moderate pulmonary hypertension , with resultant moderate pulmonary regurgitation. The plan was to proceed as soon as possible with aortic valve replacement.
Introduction:Developing multi-modal cardiopulmonary resuscitation (CPR) in animal models of cardiacarrest is challenging because of the exponential increase in the number of possible combinations of n modalities. Circulation, Volume 150, Issue Suppl_1 , Page ASa310-ASa310, November 12, 2024.
A dissection flap is noted in the intrabdominal aorta, and the aortic outflow tract is also noted to appear wider than normal. The CT angio showed a type A aortic dissection extending from the aortic root proximally to the carotid and left subclavian artery and distally to the common femoral arteries.
An elderly patient with a ruptured abdominal aortic aneurysm: Formal ECG Interpretation (final read in the chart!) : "Inferior ST elevation, lead III, with reciprocal ST depression in aVL." Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiacarrest with unrecognized STEMI, died. What do you think?
2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. Thirty-six patients (36%) presented with cardiacarrest, and 78% (28/36) underwent emergent angiography. Widespread ST-depression with reciprocal aVR ST-elevation can be cause by: Heart rate related: tachyarrhythmia (e.g., Left main? 3-vessel disease?
Category 2 : An increase in myocardial oxygen demand due to tachycardia, elevated ventricular afterload (BP or aortic stenosis), or increased wall stretch (admittedly this latter is more complicated) or a decrease in oxygen supply due to hypotension, anemia, hypoxia, or a combination of all of the above. Aortic Stenosis f.
On arrival his BP was 70s/40s, so an intra-aortic ballon pump was placed. A repeat ECG was done: Obvious anterolateral wall STEMI. Proximal LAD occlusion with dramatic ST Elevation) The patient was intubated and taken to the cath lab. They found a 100% acute thrombotic proximal LAD lesion.
1,2 ASCVD causes or contributes to conditions that include coronary artery disease (CAD), cerebrovascular disease, and peripheral vascular disease (inclusive of aortic aneurysm).3 alone, more than 800,000 of these people are at risk of MI and for approximately 200,000 of them, this may well be their second life-threatening cardiac event.
About two hours after admission, he suffered a cardiacarrest (whether it was VF/VT or PEA is not available) and expired. Chest pain and Concordant ST Depression in a patient with aortic valve and previously normal angiogram Right Bundle Branch Block and ST Depression in V1-V3. Is that normal?
These include ( among others ) — acute febrile illness — variations in autonomic tone — hypothermia — ischemia-infarction — malignant arrhythmias — cardiacarrest — and especially Hyperkalemia. Patients with such conditions that may transiently mimic the ECG findings of a Brugada-1 pattern are said to have Brugada Phenocopy.
Chugh, the Pauline and Harold Price Chair in Cardiac Electrophysiology Research at Cedars-Sinai, investigates the causes of and potential treatments for abnormal heart rhythms, including sudden cardiacarrest. Experts Available The following experts also are available for interviews throughout ACC.24: 24: Christine M.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content