This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
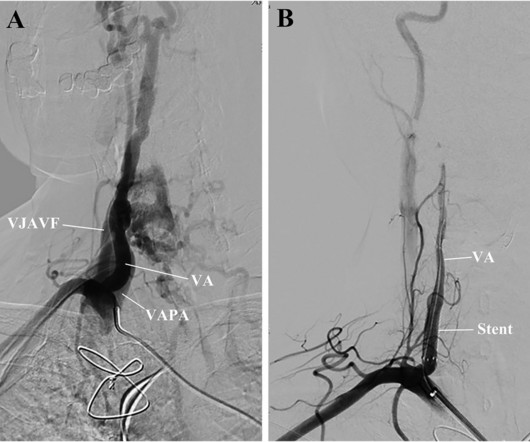
The patient, who complained of dizziness, was initially diagnosed with bradycardia and aortic paravalvular leak. However, the symptoms persisted even after permanent pacemaker implantation and transcatheter closure of the aortic paravalvular leak.
Bradycardia-dependent block is characterized by slowed or blocked conduction through His-Purkinje (HPS) fibers. We describe a case of bradycardia-dependent block after transcatheter aortic valve replacement (TAVR). We describe a case of bradycardia-dependent block after transcatheter aortic valve replacement (TAVR).
Left bundle branch block (LBBB) is a frequent complication of transcatheter aortic valve implantation (TAVI) and was shown to predict advanced atrio-ventricular block and pacemaker implantation (PI).1,2 1,2 Previous studies focused on persistent TAVI-induced LBBB. There are limited data on TAVI-related intermittent LBBB.
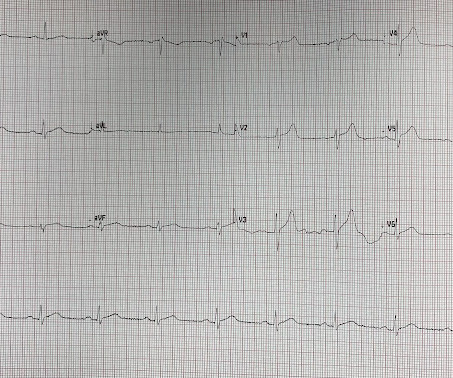
This ECG was recorded on arrival in the ED: Here is the interpretation of the conventional algorithm (Veritas): SINUS BRADYCARDIA ST ELEVATION, PROBABLY EARLY REPOLARIZATION [ST ELEVATION WITH NORMALLY INFLECTED T-WAVE] BORDERLINE ECG What do you think?
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. Limiting one's interpretation to marked bradycardia with high-grade AV block in need of pacing in this patient with multiple syncopal epiosodes — more than suffices for "the quick answer".
Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). RBBB in blunt chest trauma seems to be indicative of several RV injury. Atrial fibrillation is also a predictor of worse outcomes in this case (Alborzi). Sinus Tachycardia ( common in any trauma patient. ).
Post PCI an intra-aortic balloon pump (IABP) was placed and a combination of norepinephrine and dobutamine was needed to maintain perfusion pressures. As per Dr. Nossen — today's initial ECG ( LEFT tracing in Figure-2 ) shows sinus bradycardia with QRS widening due to bifascicular block ( RBBB/LAHB ).
Reasons for not prescibing or discontinuing were: CKD 6, severe aortic stenosis 5, asthma 3, symptomatic bradycardia 5, hypotension 3, type1 diabetes 2, syncope 1, Raynauds 1, patient choice 8 and 6 patients died before all appropriate medications could be initiated.
His first electrocardiogram ( ECG) is given below: --Sinus bradycardia. As his pain was very severe, emergency physicians concerned of aortic dissection and ordered a thoracic CT scan. Blood pressure: 130/80 mmHg, heart rate: 45/min, respiratory rate: 18/min, SaO2: %98, body temperature: normal.
Chest pain and Concordant ST Depression in a patient with aortic valve and previously normal angiogram Right Bundle Branch Block and ST Depression in V1-V3.
There was concern for aortic dissection, so a CT was done and was negative. This is sinus bradycardia. Another ECG was recorded at 35 minutes: It is hard to discern a difference At this point, the first troponin I returned at 0.55 ng/mL (significantly elevated) A D dimer was also elevated. The QRS is narrow.
Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). Sinus Tachycardia ( common in any trauma patient. ). RBBB ( as by far the most common conduction defect — owing to the more vulnerable anatomic location of the RV ).
Sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. Cardiology noted there was no STEMI criteria and the first troponin was in the normal range (25ng/L, with normal <26), so alternate diagnoses were considered and the patient was sent for CT to rule out aortic dissection. What do you think?
Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. PVCs N ot generally considered abnormal ECG findings: Isolated PAC, First Degree AV Block, Sinus bradycardia at a rate of 35-45, and Nonspecific ST-T abnormalities (even if different from a previous ECG). heart auscultation (aortic stenosis); c.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content